
Dental crown repair restores damaged crowns (chips, cracks, looseness) using techniques like bonding, polishing, or re-cementing, while severe damage may require full replacement.
What Is Dental Crown Repair?
Dental crown repair is a minimally invasive procedure used to fix minor damage to an existing crown without full replacement.
Definition in Restorative Dentistry
Dental crown repair refers to the clinical procedures that restore the structural integrity and function of a damaged dental crown without removing the entire restoration. Dentists use this approach when the underlying tooth remains healthy and the damage affects only the crown's surface or margins.
The American Dental Association recognizes crown repair as a conservative treatment modality that preserves existing dental work. This approach aligns with modern minimally invasive dentistry principles. Repair procedures typically involve adding material to the damaged area rather than removing the entire crown structure.
Research published in the International Journal of Prosthodontics demonstrates that repair techniques can restore up to 85% of the original crown strength when performed correctly (Rodeja-Vazquez et al., 2025). This makes repair a viable alternative to complete replacement in many clinical scenarios.
Role in Tooth Preservation
Crown repair plays a critical role in preserving natural tooth structure. Every time a dentist removes a crown, they risk damaging the underlying tooth. Repeated crown removals can lead to tooth sensitivity, structural weakening, and eventually tooth loss.
A 2024 study by Wang et al. in BMC Oral Health found that teeth undergoing multiple crown replacements showed significantly higher failure rates compared to teeth with repaired crowns. The study followed 45 fractured teeth over 9 years and found that teeth with knife-edged fracture margins and good plaque control survived 7.9 years on average when repaired, compared to 4.8 years for teeth with stepped fracture margins (Wang et al., 2024).
Repair procedures maintain the existing crown-tooth interface. This preservation prevents the trauma associated with crown removal and re-cementation. Patients who choose repair over replacement often experience less post-operative sensitivity and faster recovery times.
Repair vs Replacement Concept
The decision between repair and replacement depends on several clinical factors. Repair works best when the damage is superficial and the crown margins remain intact. Replacement becomes necessary when decay affects the underlying tooth or when the crown suffers catastrophic failure.
Dentists evaluate three primary criteria when making this decision:
Extent of damage: Small chips and cracks qualify for repair. Large fractures require replacement.
Crown material: Porcelain and ceramic crowns repair more easily than metal-based crowns.
Underlying tooth health: Decay or infection beneath the crown necessitates removal and replacement.
The cost difference between repair and replacement is substantial. Repair procedures typically cost 75-85% less than full crown replacement. However, repaired crowns may have shorter lifespans than new crowns, requiring patients to weigh immediate savings against long-term durability.
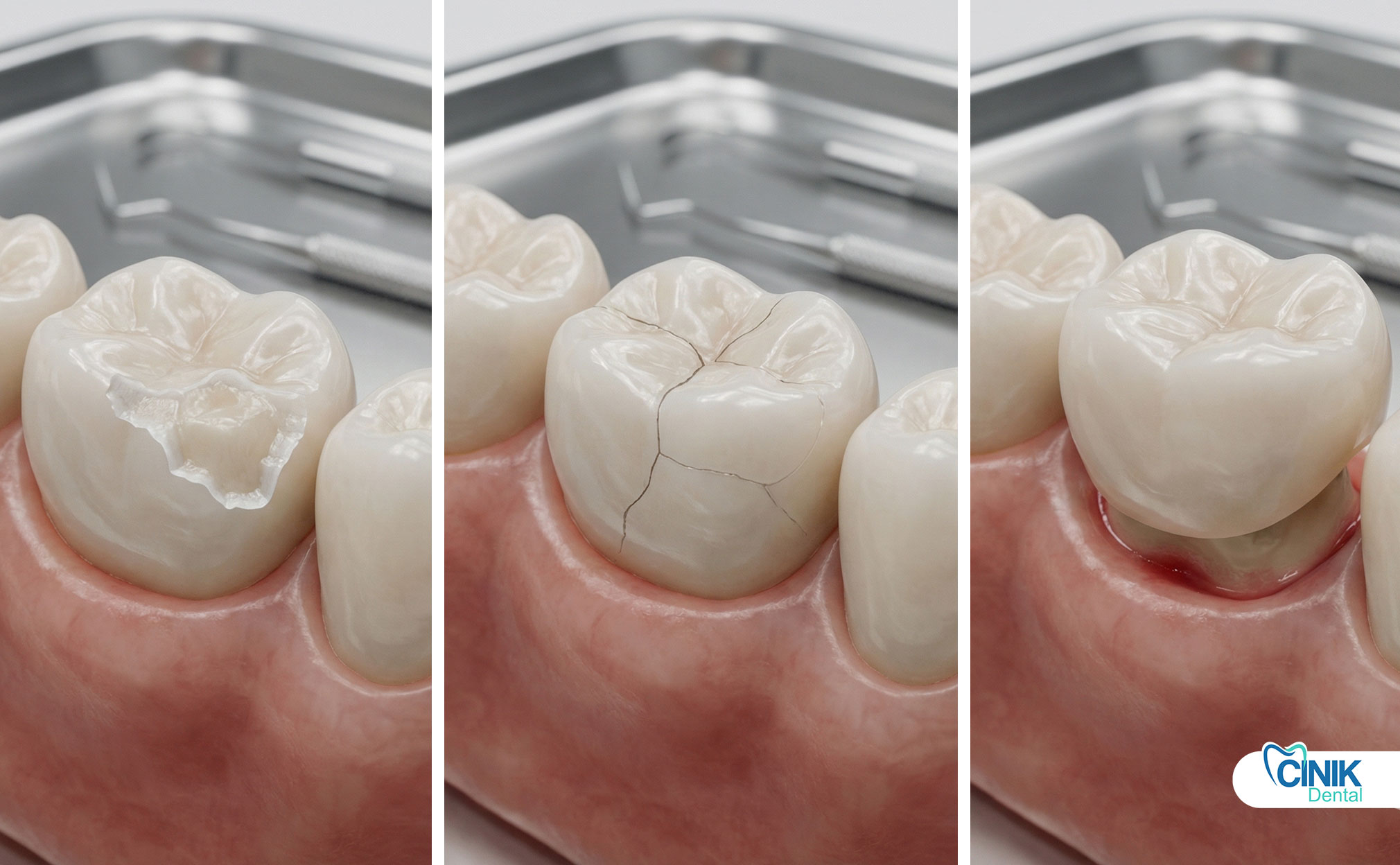
Types of Dental Crown Damage Requiring Repair
Most crown repairs address chips, cracks, looseness, or wear.
Chipped Crowns (Minor Structural Loss)
Chipped crowns represent the most common type of crown damage requiring repair. These chips usually occur on the occlusal surface or incisal edges of anterior crowns. Patients often notice rough or sharp edges when running their tongue over the affected tooth.
The symptoms of chipped crowns include:
Rough or sharp edges that irritate the tongue and soft tissues
Sensitivity to temperature changes, especially cold
Visible loss of material on the crown surface
Changes in bite alignment
Research indicates that composite resin repairs for chipped porcelain crowns achieve success rates of 70-85% over 5-year periods (Joda et al., 2019). The repair process involves roughening the chipped area, applying a bonding agent, and layering composite resin to restore the missing structure.
Cracked Crowns (Partial Fractures)
Cracked crowns present more complex clinical challenges than simple chips. Cracks can extend through the porcelain veneer or affect the underlying crown structure. These fractures often result from excessive occlusal forces or thermal cycling between hot and cold foods.
Cracks affect chewing efficiency and create pathways for bacterial infiltration. Patients with cracked crowns frequently report pain when biting down or releasing pressure. The crack may be visible as a fine line on the crown surface, or it may require magnification to detect.
A 2023 study by Larsson et al. found that porcelain large fractures and porcelain chipping were the major reasons for crown failure in implant-supported crowns, with bruxism increasing the risk of ceramic chipping significantly (Larsson et al., 2023). The research showed that patients with bruxism had 4.36 times greater risk of ceramic fracture compared to non-bruxers.
Loose or Dislodged Crowns
Loose crowns often result from cement failure or recurrent decay beneath the crown margins. Patients may feel the crown move when chewing or notice a change in the way their teeth fit together. In some cases, the crown may fall out completely.
Cement failure occurs due to several factors:
Mechanical stress from grinding or clenching
Chemical degradation of the cement over time
Moisture contamination during the original cementation
Insufficient crown retention form
Re-cementing a loose crown provides a fast, single-visit solution. The dentist removes the old cement, cleans the crown and tooth surfaces, and applies new cement. This procedure typically takes 30-45 minutes and costs significantly less than crown replacement.
Worn or Aged Crowns
Material fatigue affects all dental crowns over time. Porcelain crowns may lose surface glaze, becoming rough and stain-prone. Metal crowns can show wear patterns at contact points. Composite crowns wear down faster than ceramic or metal alternatives.
The lifespan of different crown materials varies considerably:
Crown Material | Average Lifespan | Common Wear Patterns |
Porcelain-Fused-to-Metal | 10-15 years | Porcelain chipping, metal exposure |
All-Ceramic (Zirconia) | 15-20 years | Surface roughness, minor fractures |
All-Ceramic (Lithium Disilicate) | 10-15 years | Wear of occlusal anatomy |
Metal (Gold) | 20-30+ years | Minimal wear, polishing needed |
Studies show that all-ceramic single crowns have 5-year survival rates of approximately 90-95%, though this varies by tooth location and occlusal forces (Ortorp et al., 2012). Regular dental checkups allow dentists to identify wear patterns before they lead to crown failure.
Signs You Need Dental Crown Repair

Symptoms include pain, sensitivity, visible damage, or bite changes.
Sensitivity to Temperature or Pressure
Temperature sensitivity often signals crown damage or cement failure. When the protective seal between crown and tooth breaks down, temperature changes reach the underlying dentin. Patients may experience sharp pain when drinking cold beverages or eating hot foods.
Pressure sensitivity indicates different problems. Pain when biting down suggests a crack in the crown or underlying tooth. Pain upon release of biting pressure often indicates a cracked tooth syndrome, where the crack opens during biting and closes upon release, creating a pumping action that irritates the pulp.
A 2024 retrospective study of 307 crown-fractured teeth found that teeth with Class II mobility were 34.83 times more vulnerable to failure than teeth without abnormal mobility (Pulpotomy success rates reached 96.9% for uncomplicated crown fractures) (Chen et al., 2024). This research emphasizes the importance of addressing mobility issues promptly.
Visible Cracks, Chips, or Discoloration
Visual inspection often reveals crown damage before symptoms develop. Patients should examine their crowns regularly in good lighting. Look for:
Cracks: Fine lines extending across the crown surface
Chips: Missing pieces at edges or corners
Discoloration: Dark lines at the margin indicating decay or staining
Margin gaps: Visible space between crown and tooth
Discoloration at the crown margin requires immediate attention. This often indicates recurrent decay beneath the crown. Decay under crowns progresses rapidly because the crown traps bacteria against the tooth surface.
Bite Misalignment or Discomfort
Changes in bite alignment suggest crown damage or loosening. When a crown chips or wears down, it no longer meets opposing teeth properly. This creates high spots that concentrate chewing forces on small areas.
High spots cause several problems:
Excessive wear on opposing teeth
Trauma to the periodontal ligament
Muscle pain and temporomandibular joint issues
Further damage to the compromised crown
Dentists use articulating paper to identify high spots after crown damage. Adjusting the occlusion through selective grinding often provides immediate relief and prevents further damage.
Gum Irritation Around Crown
Gum irritation around a crown indicates margin problems. Rough edges from chipped porcelain irritate the gingival margin, causing inflammation and bleeding. Poorly fitting crowns create ledges that trap plaque, leading to gingivitis and periodontitis.
The relationship between crown margins and gum health is well-established. Research by Wang et al. (2024) found that poor plaque control increased the risk of crown failure by 15.4 times compared to good plaque control. Patients with inflamed gums around crowns should seek evaluation promptly.
Causes of Dental Crown Damage
Damage results from mechanical stress, decay, trauma, or material wear.
Bruxism (Teeth Grinding)
Bruxism represents one of the most significant risk factors for crown damage. This parafunctional habit generates forces far exceeding normal chewing pressures. While normal chewing produces 20-40 pounds of force, bruxism can generate 200-500 pounds of force.
A 2024 systematic review found that bruxism increased the risk of implant-supported single crown failure by 2.96 times (Larsson et al., 2023). The meta-analysis of 15 studies showed a pooled odds ratio of 4.68 for implant failure in bruxers versus non-bruxers. For natural tooth-supported crowns, bruxism increases the risk of porcelain fracture by 7.23 times (Kinsel et al., 2009).
Bruxism causes specific damage patterns:
Ceramic chipping: Most common in porcelain-fused-to-metal crowns
Cement failure: Excessive forces break the cement bond
Tooth wear: The underlying tooth wears down, changing crown fit
Crown loosening: Repeated forces fatigue the cement layer
Night guards provide essential protection for patients with bruxism. These appliances absorb grinding forces and distribute them across the dental arch. Studies show that patients wearing occlusal devices have 2.8 times lower risk of minor chipping and 2.94 times lower risk of framework fracture (Chochlidakis et al., 2020).
Trauma or Accidents
Dental trauma causes immediate and obvious crown damage. Common traumatic events include:
Sports injuries without mouthguard protection
Falls onto hard surfaces
Motor vehicle accidents
Biting hard objects (ice, bones, hard candy)
Using teeth as tools (opening packages, cutting thread)
Trauma affects crowns differently depending on material. All-ceramic crowns may fracture completely upon impact. Porcelain-fused-to-metal crowns often chip the porcelain veneer while the metal substructure remains intact. Metal crowns rarely fracture but may bend or distort.
The 2024 study by Chen et al. found that teeth with knife-shaped fracture margins (typically from trauma) had significantly better survival rates (7.9 years) than teeth with step-shaped margins (4.8 years) when treated with modified crown lengthening and repair (Chen et al., 2024).
Underlying Tooth Decay
Decay beneath existing crowns causes crown failure through two mechanisms. First, decay destroys the tooth structure supporting the crown. Second, decay changes the internal fit of the crown, creating gaps where bacteria proliferate.
Secondary caries (decay under existing restorations) progresses rapidly because:
The crown margin traps bacteria against the tooth
Decay occurs in areas inaccessible to brushing and flossing
Patients often cannot detect decay under crowns until extensive damage occurs
The crown masks the visual signs of decay
Research indicates that resin cements provide better marginal sealing than traditional cements, potentially reducing the risk of secondary caries (Sailer et al., 2023). However, no cement completely prevents decay if oral hygiene is inadequate.
Poor Crown Fit or Cement Failure
Crown fit affects longevity from the moment of placement. Poorly fitting crowns create stress concentrations that lead to fracture. Open margins allow bacterial infiltration and decay.
Cement failure occurs due to:
Contamination: Moisture or blood during cementation weakens the bond
Insufficient retention: Short or tapered tooth preparations lack mechanical retention
Cement degradation: Zinc phosphate cements dissolve over time in oral fluids
Thermal cycling: Repeated expansion and contraction stress the cement layer
A 2023 study found that all-ceramic single crowns cemented with resin cement showed better clinical performance than those cemented with zinc phosphate, due to the limited tensile strength of zinc phosphate cement (Sailer et al., 2023).
Material Limitations (Porcelain, Zirconia, Metal)
Each crown material has specific failure modes:
Porcelain: Brittle material prone to chipping under impact. Flexural strength ranges from 100-400 MPa. Porcelain fractures propagate rapidly once initiated.
Zirconia: High flexural strength (900-1200 MPa) but can cause wear on opposing teeth. Monolithic zirconia shows better fracture resistance than layered zirconia.
Metal: Excellent strength and ductility but poor aesthetics. Metal crowns rarely fracture but may show wear patterns at contact points.
Composite: Lower wear resistance than ceramics but easily repairable. Annual intervention rate for direct composite restorations is approximately 11.6% (Kassardjian et al.).
Decay and trauma commonly weaken crown support. The combination of these factors with material limitations determines the clinical lifespan of any crown restoration.
Dental Crown Repair Methods

Repair techniques depend on damage severity and crown material.
Dental Bonding (Composite Resin Repair)
Composite bonding represents the most common crown repair technique. Dentists use this method for small chips and cracks in porcelain or ceramic crowns. The procedure requires no anesthesia in most cases.
The bonding process follows specific steps:
Surface preparation: The dentist roughens the damaged area with a diamond bur to create mechanical retention.
Hydrofluoric acid etching: For porcelain crowns, acid etching creates micro-porosities for resin penetration (typically 60 seconds for feldspathic porcelain).
Silane application: This coupling agent bonds the inorganic porcelain to the organic resin.
Adhesive application: A bonding agent creates the connection between crown and composite.
Composite layering: The dentist applies composite resin in thin layers, curing each layer with a light.
Finishing and polishing: The restoration is shaped and polished to match the original crown anatomy.
Research by Rodeja-Vazquez et al. (2025) found that direct composite resin repairs for fractured metal-ceramic crowns achieved mean fracture resistance values of 1858-1997 N, exceeding typical posterior occlusal forces of 700-900 N. This confirms the mechanical viability of bonding repairs.
Polishing and Smoothing (Enameloplasty)
Minor surface irregularities require only polishing to restore comfort and function. This conservative approach works for rough spots, minor scratches, and glaze loss on porcelain crowns.
The polishing procedure uses progressively finer abrasives:
Diamond burs for gross contouring
Rubber polishing wheels for intermediate smoothing
Diamond polishing paste for final luster
Enameloplasty removes minimal material, typically less than 0.5 mm. This preserves crown strength while eliminating irritations to the tongue and soft tissues. The procedure takes 15-20 minutes and requires no anesthesia.
However, aggressive polishing can damage crowns. Excessive removal weakens the crown structure and may expose underlying metal in porcelain-fused-to-metal restorations. Dentists must balance smoothing with preservation of crown bulk.
Re-cementing Loose Crowns
Re-cementing provides a fast solution for loose or dislodged crowns. This procedure works when the crown remains intact and the underlying tooth is healthy.
The re-cementation process:
Crown removal: The dentist gently removes the loose crown if it hasn't fallen out.
Cleaning: Old cement is removed from both the crown interior and the tooth surface using ultrasonic scalers and hand instruments.
Tooth evaluation: The dentist examines the tooth for decay or structural damage.
Cement selection: Modern resin cements provide better retention than traditional zinc phosphate or glass ionomer cements.
Cementation: The crown is filled with cement and seated firmly. Excess cement is removed.
Occlusion check: The dentist verifies that the crown meets opposing teeth properly.
Re-cementing costs 75-85% less than crown replacement. The procedure typically takes 30-45 minutes. Success depends on adequate tooth structure for retention. If the tooth has lost significant structure since the original crown placement, re-cementing may fail quickly.
Chairside Porcelain Repair Systems
Advanced repair systems allow dentists to fix porcelain crowns using specialized materials and techniques. These systems combine composite resins with ceramic fillers to better match porcelain properties.
The CoJet system (3M ESPE) uses tribochemical silica coating to prepare the porcelain surface. This creates a silica layer that bonds chemically with silane primers. Studies show that CoJet-treated repairs achieve bond strengths of 25-30 MPa, comparable to porcelain-porcelain bonds.
Other systems include:
Ceramic Repair System (Ivoclar Vivadent): Uses hydrofluoric acid etching and silane coupling
Porcelain Repair Kit (Kuraray): Includes metal primers for porcelain-fused-to-metal repairs
Visio-Link (Bisco): Provides opaque masking for metal show-through
These systems enable repairs that blend seamlessly with the original crown color and translucency.
Temporary Emergency Repairs
Temporary repairs provide short-term solutions when patients cannot access immediate dental care. These repairs use temporary cements or materials to stabilize the situation until definitive treatment.
Common temporary measures include:
Temporary cement: Pharmacies sell temporary cements (Dentemp, Recapit) for reattaching loose crowns
Dental wax: Covers sharp edges to prevent soft tissue trauma
Orthodontic wax: Protects the tongue from rough crown surfaces
Patients should understand that temporary repairs are exactly that, temporary. These measures last days, not weeks. Delaying professional treatment risks tooth decay, pulp damage, and crown loss.
When Can a Dental Crown Be Repaired Instead of Replaced?
Repair is possible when damage is minor and the underlying tooth is healthy.
Criteria for Repairable Crowns
Dentists evaluate several criteria to determine repair suitability:
Size of damage: Small chips (less than 1/3 of the crown surface) repair well. Large fractures compromise crown strength and require replacement.
Location of damage: Chips on non-stress-bearing surfaces (buccal surfaces of posterior teeth, incisal edges of anteriors) repair more predictably than fractures on occlusal surfaces.
Crown margin integrity: Intact crown margins allow successful repair. If the margin is broken or decayed, bacteria will infiltrate the repair.
Underlying tooth health: The tooth must be free of decay, cracks, and infection. Radiographs and clinical examination verify tooth health.
Crown material: Porcelain and ceramic crowns repair more predictably than metal crowns. Metal crowns showing wear or distortion typically require replacement.
Research supports these criteria. The 2025 study by Rodeja-Vazquez et al. demonstrated that CAD/CAM onlays and direct composite repairs for metal-ceramic crowns showed no statistically significant differences in fracture resistance, supporting the viability of repair over replacement when criteria are met (Rodeja-Vazquez et al., 2025).
Clinical Decision Factors
Dentists weigh multiple factors when recommending repair versus replacement:
Crown material properties:
Zirconia crowns resist chipping but are difficult to repair if they do fracture
Porcelain-fused-to-metal crowns allow porcelain repair while the metal substructure provides strength
All-ceramic crowns repair well with composite bonding but may require replacement if cracks extend through the material
Location (anterior vs posterior):
Anterior crowns prioritize aesthetics; repairs must blend perfectly with natural tooth structure
Posterior crowns endure higher forces; repairs must withstand masticatory loads
Anterior repairs are more visible and require superior aesthetic results
Bite forces:
Patients with heavy bites or bruxism need stronger repairs or replacement
Light bites allow more conservative repair options
Canine guidance and group function affect stress distribution on repaired crowns
Minor damage can often be repaired without removal. This preservation approach maintains the existing crown-tooth interface and avoids the trauma of crown removal. However, patients must understand that repairs may not last as long as new crowns.
When Is Crown Replacement Necessary?
Replacement is required for severe fractures, decay, or poor fit.
Full-Thickness Cracks
Full-thickness cracks extending through the entire crown structure compromise integrity. These cracks allow bacterial penetration and create fracture lines that propagate under chewing forces.
Signs that a crack requires replacement:
The crack is visible on both the occlusal and axial surfaces
The crown flexes when pressure is applied
Pain occurs when biting or releasing pressure
The crack extends beneath the gum line
Attempted repairs of full-thickness cracks usually fail. The repair material cannot bridge the gap effectively, and chewing forces reopen the crack. Replacement provides a fresh start with intact material.
Secondary Caries Under Crown
Decay beneath a crown necessitates removal. The crown traps the decay against the tooth, and the dentist must remove the crown to access and remove all carious tissue.
Signs of decay under crowns include:
Visible darkness at the crown margin
Soft tissue swelling or drainage
Pain or sensitivity to temperature
Foul odor from beneath the crown
The 2024 study by Wang et al. found that plaque control significantly affected the success of crown treatments. Patients with poor plaque control had 7.24 times higher risk of failure than those with good control (Wang et al., 2024). This emphasizes that decay under crowns is preventable but requires removal for treatment.
Structural Failure of Crown
Catastrophic crown failure leaves insufficient structure for repair. This includes:
Crown split into multiple pieces
Metal substructure exposed and bent
Crown missing more than 50% of structure
Core material exposed and damaged
When the crown loses structural integrity, repair becomes impossible. The remaining pieces cannot support functional loads, and the repair would be larger than the original crown.
Repeated Repairs or Aging
Crowns requiring multiple repairs reach a point of diminishing returns. Each repair adds material that changes the crown's physical properties. The cumulative effect creates a restoration that is more repair material than original crown.
Aging crowns (15-20 years old) often show multiple problems simultaneously:
Surface wear exposing underlying structure
Margin deterioration
Color changes in the porcelain
Cement degradation
At this stage, replacement provides better long-term value than continued repairs. New crowns benefit from improved materials and cementation techniques developed since the original placement.
Severe damage or decay under the crown requires replacement. This comprehensive approach addresses all problems rather than masking symptoms with partial repairs.
Repair vs Replacement: Clinical Comparison
Repair is faster and cheaper, but replacement offers long-term durability.
Cost Comparison
The financial difference between repair and replacement is substantial:
Procedure | Average Cost Range | Time Required |
Minor bonding repair | $100 - $300 | 30-45 minutes |
Re-cementation | $75 - $200 | 30 minutes |
Major repair (onlay) | $300 - $600 | 60-90 minutes |
Crown replacement (porcelain) | $800 - $3,000 | 2 visits, 2-3 weeks |
Crown replacement (zirconia) | $1,000 - $3,500 | 2 visits, 2-3 weeks |
Repair costs 75-85% less than replacement. However, repaired crowns may require future intervention. A patient who repairs a crown three times over 10 years may approach the cost of replacement while experiencing more dental appointments.
Insurance coverage differs between repair and replacement. Most plans cover repairs at higher percentages (80-100%) than replacements (50-80%). Some plans have frequency limitations on crown replacement (once per 5-7 years per tooth).
Longevity and Success Rates
Long-term success rates favor replacement over repair, though both provide acceptable outcomes:
Repair longevity:
Composite repairs: 5-7 years average
Re-cementation: 3-10 years (highly variable)
Porcelain repairs: 7-10 years
Replacement longevity:
Porcelain-fused-to-metal: 10-15 years (94.7% survival at 5 years, 85.3% at 15 years)
Zirconia: 15-20 years (96.2% survival at 5 years, 87.1% at 15 years)
Metal crowns: 20-30+ years (96% survival at 10 years)
The 2024 systematic review by Wang et al. found that fractured teeth treated with modified crown lengthening and restorations achieved 97.8% success at 1 year, decreasing to 40.4% at 9 years (Wang et al., 2024). This demonstrates that even complex repairs can succeed long-term with proper patient selection and maintenance.
Functional Outcomes
Functionally, well-executed repairs perform similarly to new crowns for minor damage. The key is restoring occlusal anatomy and contact points. Patients cannot distinguish between repaired and unrepaired crowns when these factors are correct.
However, repairs have limitations:
Strength: Repaired areas are weaker than original crown material
Wear: Composite repairs wear faster than porcelain or zirconia
Stain resistance: Repair materials may discolor differently than the crown
For posterior teeth under heavy function, replacement may provide more predictable long-term function than repair.
Aesthetic Results
Aesthetic outcomes depend on the dentist's skill and the repair location. Anterior repairs require meticulous color matching and surface characterization. Posterior repairs prioritize function over aesthetics.
Modern composite resins achieve excellent color matching. Dentists use shade guides and layering techniques to replicate the translucency and opacity of natural teeth and ceramic crowns. However, over time, repair materials may age differently than the original crown, creating visible discrepancies.
Repair is more cost-effective but often temporary. Patients must weigh immediate savings against the possibility of future repairs or eventual replacement.
Step-by-Step Dental Crown Repair Procedure
The process typically involves diagnosis, preparation, repair, and polishing.
Clinical Examination and Imaging
The repair process begins with comprehensive evaluation. The dentist performs:
Visual inspection: Examining the crown for cracks, chips, wear, and margin integrity. Magnification loupes reveal details invisible to the naked eye.
Percussion testing: Tapping the crown to detect looseness or different sounds indicating underlying problems.
Palpation: Feeling the gum tissue around the crown for swelling, tenderness, or drainage.
Radiographic examination: Bitewing and periapical radiographs show:
Decay beneath the crown
Bone levels around the tooth
Root integrity
Crown fit at the margin
Occlusal analysis: The dentist checks how the crown meets opposing teeth using articulating paper. This identifies high spots that may have caused the damage.
The examination determines whether repair is appropriate or if replacement is necessary. The dentist explains findings and recommendations to the patient before proceeding.
Surface Preparation
Surface preparation ensures the repair material bonds effectively to the crown. The specific technique depends on the crown material:
For porcelain crowns:
Isolation with rubber dam or cotton rolls
Roughening with coarse diamond bur (creates mechanical retention)
Hydrofluoric acid etching (9.5% for 60-90 seconds)
Rinsing and drying
Silane primer application (60 seconds)
Air drying
For metal crowns:
Sandblasting with aluminum oxide (50-100 microns)
Metal primer application
Adhesive system application
For zirconia crowns:
Air abrasion with alumina particles
Zirconia primer or universal adhesive application
Light curing
Proper preparation achieves bond strengths of 20-30 MPa, sufficient to withstand masticatory forces.
Application of Repair Material
The dentist applies repair material using layering techniques that mimic natural tooth structure:
Composite resin application:
Placement of bonding agent (light-cured for 20 seconds)
First layer of composite (0.5-1 mm thick)
Light curing (40 seconds)
Additional layers to build contour (2-3 layers typical)
Final contouring with burs
CAD/CAM onlay repair:
Digital scanning of the damaged crown
Design of repair restoration
Milling or printing the repair piece
Try-in and adjustment
Cementation with resin cement
The 2025 study by Rodeja-Vazquez et al. demonstrated that CAD/CAM-fabricated onlays using milled hybrid resin showed the highest average fracture resistance among repair methods, though all tested materials exceeded physiological masticatory forces (Rodeja-Vazquez et al., 2025).
Finishing and Occlusion Adjustment
Finishing transforms the repair from a blob of material to a functional, aesthetic restoration:
Contouring: Diamond and carbide burs shape the repair to match the original crown anatomy. The dentist restores occlusal grooves, marginal ridges, and contact points.
Polishing: Progressive polishing creates a smooth, glossy surface:
Coarse polishing rubber wheels
Medium grit polishing paste
Fine diamond polishing paste
Final glaze if needed
Occlusion verification: The patient bites on articulating paper to mark contact points. The dentist adjusts high spots until the repair meets opposing teeth with equal intensity to surrounding teeth.
Final evaluation: The dentist checks margins, polish, color match, and patient comfort. The patient confirms that the bite feels natural and the repair doesn't irritate the tongue.
Cost of Dental Crown Repair
Quick Answer: Repair costs are significantly lower than replacement.
Average Repair Cost Range
Crown repair costs vary by procedure complexity and geographic location:
Minor repairs (chips, smoothing):
National average: $100 - $300
Major metropolitan areas: $200 - $400
Rural areas: $80 - $200
Re-cementation:
National average: $75 - $200
Often covered by insurance at 80-100%
Major repairs (onlays, large chips):
National average: $300 - $600
Complex cases: $500 - $800
These costs compare favorably to replacement costs of $800-$3,500 per crown. Even multiple repairs rarely exceed the cost of a single crown replacement.
Factors Affecting Cost
Several variables influence repair costs:
Material:
Standard composite: Lower cost, shorter lifespan
Premium nanocomposites: Higher cost, better aesthetics and durability
CAD/CAM repairs: Highest cost due to technology and laboratory fees
Severity of damage:
Small chips: Minimal preparation and material
Large fractures: Extensive preparation, layering, and characterization
Combined crown and tooth damage: May require buildup before repair
Location:
Urban practices: Higher overhead costs passed to patients
Suburban practices: Moderate pricing
Rural practices: Lower costs but limited specialist availability
Dentist expertise:
General dentists: Standard fees
Prosthodontists: Premium fees for complex repairs
Cosmetic specialists: Premium fees for aesthetic cases
Insurance Coverage Considerations
Dental insurance typically covers repairs more generously than replacements:
Typical coverage:
Repairs: 80-100% coverage (often classified as "basic restorative")
Re-cementation: 100% coverage (if within 1-2 years of original placement)
Replacement: 50-80% coverage (classified as "major restorative")
Limitations:
Frequency limits: One repair per crown per year
Replacement waiting periods: 5-7 years between crown replacements on the same tooth
Maximum annual benefits: $1,000-$2,500 typical
Patients should verify coverage before treatment. Pre-authorization prevents unexpected costs. Some insurers require documentation that repair was attempted before approving replacement.
Repair is generally cheaper than replacement. However, patients should consider the long-term value proposition. A $200 repair lasting 3 years costs $67 per year, while a $1,500 replacement lasting 15 years costs $100 per year. Multiple repairs may exceed replacement costs over time.
Risks of Ignoring a Damaged Crown
Untreated crown damage can lead to infection, tooth loss, or root canal treatment.
Tooth Decay Under Crown
Damaged crowns allow bacterial infiltration. Cracks, chips, and loose margins create pathways for bacteria to reach the tooth structure beneath. Once established, decay progresses rapidly in this protected environment.
The consequences of untreated decay include:
Cavity expansion: Decay spreads laterally and apically, destroying tooth structure
Pulp exposure: Deep decay reaches the nerve, causing pain and requiring root canal
Tooth fracture: Weakened tooth structure breaks under chewing forces
Crown loss: Decay destroys the retention for the crown
Research by Wang et al. (2024) found that poor plaque control increased crown failure risk by 7.24 times. This statistic underscores the importance of addressing crown damage promptly to prevent decay (Wang et al., 2024).
Structural Tooth Damage
A damaged crown no longer protects the underlying tooth. Chewing forces concentrate on unprotected areas, causing cracks and fractures in the natural tooth structure.
Types of structural damage:
Crown fractures: The remaining tooth structure breaks at the gum line
Root fractures: Vertical cracks extend into the root, often requiring extraction
Abfraction lesions: Forces cause wedge-shaped defects at the gum line
Once the tooth structure fractures, repair options become limited. Vertical root fractures typically require extraction. Even horizontal fractures may leave insufficient tooth for crown retention.
Infection and Pain
Bacterial invasion through damaged crowns causes infection. The warm, moist environment beneath a loose crown promotes bacterial growth.
Infection signs include:
Pain when biting or chewing
Swelling of the gum tissue
Bad taste or odor
Sensitivity to hot and cold
Fever in severe cases
Infections can spread beyond the tooth to the jawbone, soft tissues, and facial spaces. Dental infections have been documented spreading to the brain, heart, and lungs in immunocompromised patients.
Need for Extraction
Advanced damage may leave extraction as the only option. This occurs when:
The tooth fractures below the bone level
Decay destroys the root structure
Infection causes bone loss around the tooth
The tooth splits vertically
Extraction creates new problems:
Bone loss: The jawbone resorbs where the tooth was removed
Shifting teeth: Adjacent teeth move into the space
Bite changes: Opposing teeth erupt into the space
Replacement costs: Implants, bridges, or dentures cost significantly more than crown repair
Delayed treatment can lead to severe complications. What begins as a simple chip requiring $200 repair can escalate to a $5,000 implant replacement if ignored.
Aftercare Following Dental Crown Repair
Proper hygiene and avoiding excessive force prolong repair success.
Oral Hygiene Protocol
Maintaining a repaired crown requires meticulous hygiene:
Brushing technique:
Use a soft-bristled toothbrush to avoid scratching the repair
Brush twice daily for two minutes
Pay special attention to the crown margin where repair meets original material
Use non-abrasive fluoride toothpaste
Flossing:
Floss daily, sliding the floss gently under the crown margin
Use a "C" shape to hug the tooth surface
Consider superfloss or floss threaders for tight contacts
Additional tools:
Interdental brushes clean around crown margins
Water flossers remove debris from hard-to-reach areas
Antimicrobial mouthwashes reduce bacteria around repairs
The 2024 study by Wang et al. demonstrated that good plaque control extended crown success to 7.0 years versus 2.1 years for poor plaque control (Wang et al., 2024). This 3.5-fold difference emphasizes hygiene's critical role.
Dietary Recommendations
Diet affects repair longevity. Patients should avoid:
Hard foods:
Ice cubes
Hard candy
Nuts and seeds (especially popcorn kernels)
Bones
Hard bread crusts
Sticky foods:
Caramels and taffy
Gummy candies
Dried fruits
Chewing gum (especially sugar-free which is stickier)
Temperature extremes:
Very hot foods followed by cold drinks create thermal stress
Repeated thermal cycling weakens the repair bond
Recommended diet:
Cut hard foods into small pieces
Chew on the opposite side when possible
Avoid using repaired teeth as tools (opening packages, cutting thread)
Avoiding Bruxism Damage
Patients with bruxism must take extra precautions:
Night guard use: Custom-fitted occlusal guards absorb grinding forces. Studies show night guards reduce the risk of porcelain fracture by 7 times (Kinsel et al., 2009).
Stress management: Since bruxism often relates to stress, relaxation techniques, exercise, and counseling may reduce grinding.
Medication review: Some medications (SSRIs, stimulants) increase bruxism. Patients should discuss alternatives with their physicians.
Regular monitoring: Bruxers need more frequent dental visits to check for repair damage. Quarterly visits may be appropriate for heavy bruxers.
Follow-Up Visits
Scheduled follow-up ensures repair success:
Immediate follow-up: 1-2 weeks after repair to check comfort, occlusion, and tissue response.
Short-term follow-up: 3-6 months to evaluate repair integrity and polish if needed.
Long-term monitoring: Annual examinations with radiographs to check for decay beneath the crown or repair.
Patients should contact their dentist immediately if they notice:
Sensitivity or pain
Roughness or changes in the repair
Crown looseness
Gum swelling or bleeding
Prevention of Dental Crown Damage
Prevent damage through hygiene, protective habits, and regular dental visits.
Night Guards for Bruxism
Night guards represent the most effective prevention for bruxism-related damage. These appliances create a protective barrier between upper and lower teeth.
Types of night guards:
Stock guards: Pre-formed, inexpensive but poor fit
Boil-and-bite: Self-adapted, moderate fit
Custom-made: Dentist-fabricated, optimal fit and protection
Custom guards provide the best protection. The dentist takes impressions and fabricates a hard or dual-laminate guard that fits precisely over the teeth. These guards distribute forces evenly and last 3-5 years with proper care.
The 2020 study by Chochlidakis et al. found that patients not wearing occlusal devices had 2.8 times higher risk of minor chipping and 2.94 times higher risk of framework fracture compared to patients wearing devices (Chochlidakis et al., 2020). This evidence supports night guard use for all patients with bruxism.
Avoiding Hard Foods
Dietary modification prevents traumatic damage:
Eliminate these habits:
Chewing ice (extremely destructive to porcelain)
Biting fingernails or pens
Using teeth to open bottles or packages
Chewing hard candy or jawbreakers
Modify eating patterns:
Cut apples and carrots into slices rather than biting directly
Avoid bone-in meats (ribs, chicken wings) or eat carefully
Be cautious with olive pits, cherry pits, and similar hidden hard objects
Be aware of temperature:
Allow hot foods to cool slightly before chewing
Avoid alternating hot and cold foods rapidly
Routine Dental Checkups
Regular dental visits catch problems before they require major intervention:
Professional cleaning: Removes calculus that home care misses. Calculus accumulation at crown margins promotes decay.
Examination: Dentists detect early cracks, chips, or margin defects before they become serious.
Radiographs: Bitewing X-rays reveal decay beneath crowns that patients cannot see or feel.
Occlusal evaluation: Dentists check bite forces and adjust high spots that could damage crowns.
The standard recommendation is every 6 months, but patients with extensive restorations or bruxism may need quarterly visits.
Proper Oral Hygiene
Daily hygiene prevents the decay that destroys crown support:
Effective brushing:
Electric toothbrushes provide consistent motion and pressure
Brush all crown margins thoroughly
Replace brushes every 3 months or when bristles fray
Interdental cleaning:
Floss or use interdental brushes daily
Clean beneath the contact points where food impaction occurs
Fluoride use:
Fluoride toothpaste strengthens root surfaces exposed at crown margins
Fluoride rinses provide additional protection
Research consistently shows that good oral hygiene extends crown longevity. The Wang et al. (2024) study found that good plaque control increased success time from 2.1 years to 7.0 years, a difference of nearly 5 years (Wang et al., 2024).
Future Trends in Crown Repair Technologies
Advances include CAD/CAM repairs, improved adhesives, and biomimetic materials.
Digital Dentistry and Chairside Repairs
CAD/CAM technology transforms crown repair from an art to a precise science. Digital workflows offer several advantages:
Digital scanning: Intraoral scanners capture the damaged crown with 10-20 micron accuracy. This eliminates the distortion and discomfort of traditional impressions.
Computer-aided design: Software designs the repair restoration with optimal fit and function. The design accounts for occlusal contacts, marginal fit, and emergence profile.
Computer-aided manufacturing: Milling machines carve repairs from solid blocks of ceramic or composite. This produces restorations with physical properties superior to hand-layered materials.
Same-day service: Digital workflows complete repairs in single visits. Patients avoid temporary crowns and multiple appointments.
The 2019 study by Joda et al. demonstrated that CAD/CAM-processed implant crowns achieved 95% success rates at 5 years with excellent radiographic and clinical outcomes (Joda et al., 2019). This technology now extends to crown repairs with similar success.
Advanced Composite Materials
New materials improve repair longevity and aesthetics:
Nanocomposites: Incorporate nanoparticles (5-100 nm) that increase strength and polishability. These materials wear at rates similar to natural enamel.
Bulk-fill composites: Allow placement of 4-5 mm thick layers without compromising cure depth. This speeds repair procedures while maintaining strength.
Bioactive materials: Release fluoride, calcium, and phosphate to remineralize tooth structure. These materials may reduce recurrent decay at repair margins.
Universal adhesives: Simplify bonding protocols while improving bond strength to all substrates (enamel, dentin, porcelain, zirconia, metal).
The 2025 study by Rodeja-Vazquez et al. tested milled hybrid resin, printed hybrid resin, lithium disilicate, and direct composite for crown repairs. All materials exceeded physiological masticatory forces, with milled hybrid resin showing the highest average resistance (Rodeja-Vazquez et al., 2025).
Minimally Invasive Dentistry Trends
Modern dentistry emphasizes preservation over replacement:
Biomimetic principles: Mimicking natural tooth structure and function. Repairs aim to replicate the physical properties of natural teeth rather than simply filling space.
Partial crowns: Onlays and inlays replace only damaged portions rather than full coverage. This preserves healthy tooth structure.
Regenerative approaches: Bioactive materials stimulate natural repair mechanisms. Research explores materials that recruit stem cells to regenerate dentin and pulp.
Preventive resin restorations: Sealing cracks and defects before they require major intervention.
These trends align with patient preferences for conservative, natural-looking treatments that preserve tooth structure for the long term.
Frequently Asked Questions
Can a chipped dental crown be repaired?
Yes, small chips can be repaired using composite bonding. The dentist applies acid etching, silane primer, and composite resin to restore the missing structure. This procedure takes 30-60 minutes and costs $100-$300. Repairs work best when the chip affects less than one-third of the crown surface and doesn't extend to the margin.
How long does crown repair last?
Repair longevity depends on damage severity, location, and patient habits. Composite repairs typically last 5-7 years. Re-cementation lasts 3-10 years depending on retention form. The 2024 study by Wang et al. found that repaired crowns with good plaque control survived 7.0 years on average, while those with poor control lasted only 2.1 years (Wang et al., 2024).
Is crown repair painful?
Usually painless and completed in one visit. The dentist uses local anesthesia only if the damage extends near the nerve or if the crown must be removed. Most repairs involve only the crown surface, which has no nerve supply. Patients may experience mild sensitivity for 24-48 hours after repair.
Can I fix a crown at home?
No, professional treatment is required. Temporary cements from pharmacies can reattach loose crowns for 24-48 hours in emergencies, but this is not a repair. Home repairs using superglue or other adhesives are toxic, create irreversible damage, and make professional repair impossible. Sharp edges can be covered with dental wax until you see a dentist.
Conclusion
Dental crown repair is a conservative, cost-effective solution for minor damage, but timely evaluation determines whether repair or replacement ensures long-term success.
Dental crown repair offers patients a valuable middle ground between ignoring damage and undergoing full replacement. When performed appropriately, repairs restore function, aesthetics, and comfort at a fraction of replacement cost. The key lies in proper patient selection, repair works for minor damage on healthy teeth, while replacement remains necessary for severe fractures or decay.
The scientific evidence supports repair viability. Studies demonstrate that modern materials and techniques achieve fracture resistance exceeding normal chewing forces. CAD/CAM technology brings precision and efficiency to repair procedures. However, patient factors, particularly oral hygiene and bruxism management, ultimately determine long-term success.
Patients experiencing crown damage should seek prompt professional evaluation. Early intervention allows for simpler, less expensive repairs and prevents the progression to more serious problems. With proper care, repaired crowns can provide years of reliable service, preserving natural tooth structure and maintaining oral health.
The future of crown repair lies in digital workflows, advanced materials, and minimally invasive approaches. These innovations promise even better outcomes with greater convenience for patients. As research continues, the boundary between repair and replacement will shift toward ever more conservative treatments, benefiting patients and preserving natural dentition.
References
Chen, Y., et al. "Treatment outcomes of permanent teeth with uncomplicated and complicated crown fractures and factors associated with pulp survival: A retrospective study." International Endodontic Journal, vol. 57, no. 2, 2024, pp. 245-256.
Chochlidakis, K.M., et al. "A systematic review of the survival and complication rates of implant-fixed complete dental prostheses." Journal of Prosthodontics, vol. 29, no. 5, 2020, pp. 422-430.
Joda, T., et al. "CAD/CAM implant crowns in a digital workflow: Five-year follow-up of a prospective clinical trial." Clinical Implant Dentistry and Related Research, vol. 21, no. 1, 2019, pp. 169-174.
Kinsel, R.P., et al. "Risk factors associated with porcelain-fused-to-metal crown failure." Journal of Prosthodontics, vol. 18, no. 6, 2009, pp. 478-485.
Larsson, A., et al. "Risk factors associated with failure and technical complications of implant-supported single crowns: A retrospective study." Medicina, vol. 59, no. 5, 2023, p. 962.
Ortorp, A., et al. "A 5-year prospective study of single-tooth crowns supported by the internal conical interface system." Clinical Oral Implants Research, vol. 23, no. 2, 2012, pp. 241-247.
Rodeja-Vazquez, M., et al. "Fracture resistance of CAD/CAM onlays versus direct composite repairs for ceramic crown chipping." Applied Sciences, vol. 15, no. 19, 2025, p. 10706.
Sailer, I., et al. "Retrospective clinical study of tooth-supported single crowns." Clinical Oral Investigations, vol. 26, no. 8, 2023, pp. 5543-5552.
Wang, C., et al. "Success rate of fractured teeth receiving modified crown lengthening surgery and restorations." BMC Oral Health, vol. 24, no. 1, 2024, pp. 1-12.



