
Gingival esthetics refers to the visual harmony of gum tissues within your smile framework. Your gums frame your teeth like a picture frame surrounds artwork. When gums look healthy, symmetrical, and properly positioned, they enhance your smile. When they don't, even perfect teeth can appear unattractive. Modern dentistry now treats "pink esthetics" with the same importance as "white esthetics" (your teeth). This shift represents one of the biggest advances in smile design over the past two decades (Chu, 2007).
What Are the Biological Foundations of Gingival Esthetics?
Your gingival tissues serve both protective and visual functions. Understanding their biology helps you appreciate why some smiles look naturally beautiful while others need enhancement.
How Does Healthy Gingiva Look and Function?
Healthy gum tissue displays specific characteristics that signal both health and beauty. The color ranges from pale pink to coral, depending on your skin tone and vascularization. The surface shows stippling, a textured appearance similar to an orange peel. The margins form knife-edged contours that scallop gracefully around each tooth. These tissues feel firm to touch and resist bleeding during brushing or probing (Newman et al., 2015).
Characteristics of Healthy vs. Unhealthy Gingiva
Feature | Healthy Gingiva | Unhealthy Gingiva |
Color | Pale pink/coral | Red, purple, or pale white |
Texture | Stippled, firm | Smooth, shiny, spongy |
Margin contour | Knife-edged, scalloped | Rolled, blunted, or receded |
Bleeding | Absent | Present on probing |
Position | Coronal to cementoenamel junction | Apical to cementoenamel junction |
The connective tissue beneath your gums contains collagen fibers that anchor the tissue to both the tooth and underlying bone. This attachment creates the biologic width, a critical zone measuring approximately 2.04 mm that maintains the seal between your tooth and gum tissue. Violating this space with restorations triggers inflammation and recession (Gargiulo et al., 1961).
What Is Gingival Biotype and Why Does It Predict Treatment Outcomes?
Your gingival biotype falls into two main categories: thick and thin. This classification predicts how your gums respond to dental procedures, trauma, and inflammation.
Thick Biotype: You have dense, fibrotic tissue with a flat architecture. This biotype shows greater resistance to recession and better healing after surgical procedures. Your underlying bone tends to be thicker with more pronounced bony architecture. Thick biotypes forgive minor surgical errors and tolerate restorative margins well (Seibert & Lindhe, 1989).
Thin Biotype: You possess delicate, translucent tissue with a highly scalloped contour. This biotype looks elegant but proves fragile. You face higher risks of gingival recession following tooth brushing trauma, orthodontic movement, or restorative procedures. Your thin tissue reveals underlying tooth color or implant grayness more readily. Thin biotypes demand meticulous surgical technique and careful restorative margin placement (Müller et al., 2000).
Comparison: Thick vs. Thin Gingival Biotypes
Parameter | Thick Biotype | Thin Biotype |
Tissue density | Dense, fibrotic | Delicate, translucent |
Surface texture | Stippled, opaque | Smooth, shiny |
Architectural form | Flat, thick scalloping | Highly scalloped, thin |
Recession risk | Low | High |
Surgical tolerance | Forgiving | Unforgiving |
Esthetic outcome | Stable but less refined | Elegant but fragile |
Common facial type | Square, strong chin | Tapered, delicate features |
How Does Periodontal Health Directly Impact Your Smile Esthetics?
Inflammation destroys the very architecture that creates beautiful smiles. When bacteria accumulate at your gumline, they trigger an immune response that breaks down collagen and bone. This process creates several esthetic disasters:
Gingival enlargement: Your gums swell, covering more tooth structure and creating a "gummy" appearance
Recession: Your gumline moves apically, exposing root surfaces and creating sensitivity
Papilla loss: The triangles of gum between your teeth shrink, leaving black spaces
Color changes: Inflammation shifts tissue from pink to red or purple hues
Maintaining periodontal health through proper hygiene and regular professional care represents your first and most important step toward gingival esthetics (Lang & Bartold, 2018).
What Are the Key Parameters That Define Gingival Esthetics?
Dental professionals measure specific landmarks when evaluating your gum esthetics. These parameters provide objective standards for diagnosis and treatment planning.
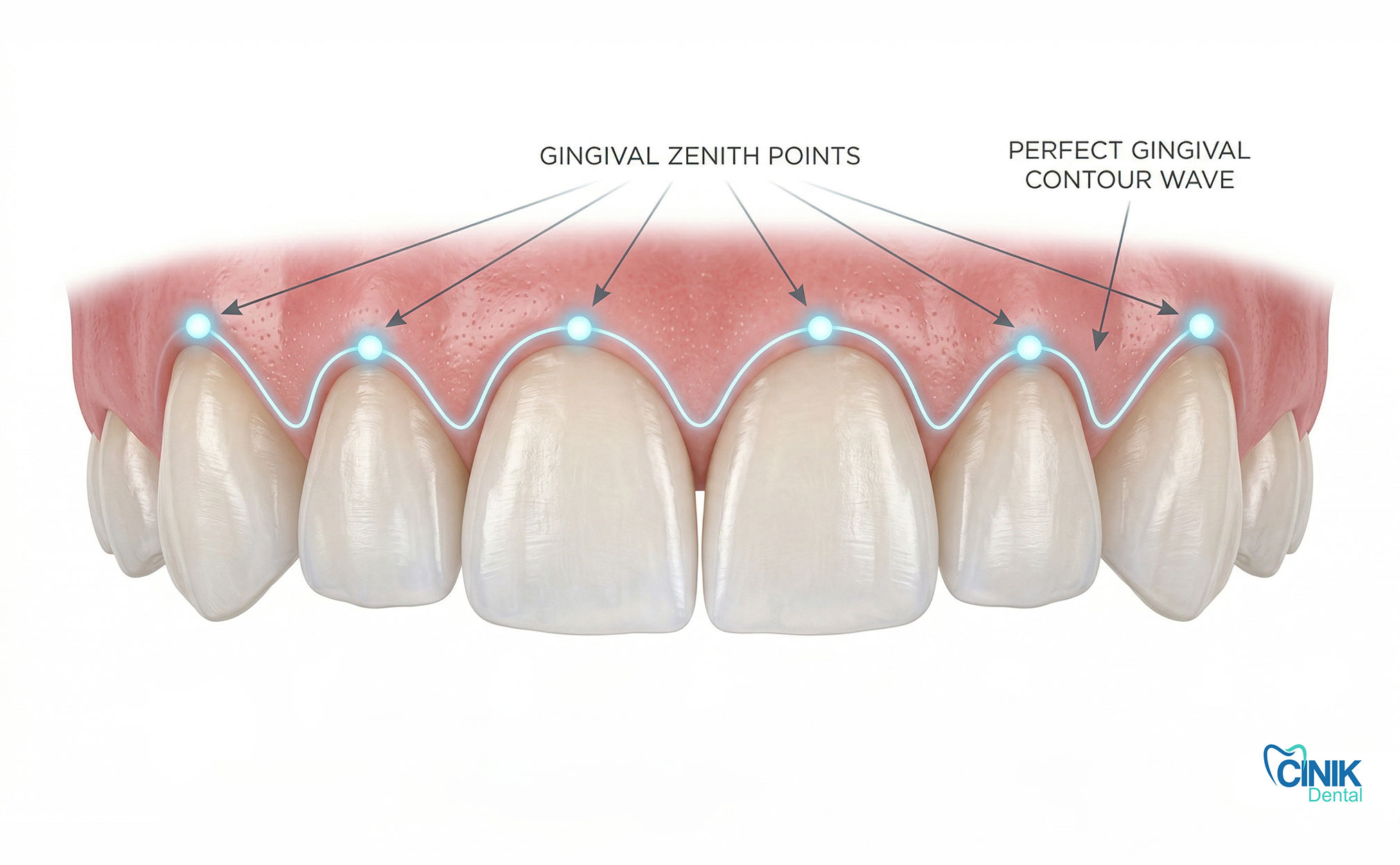
Where Should Your Gingival Zenith Position Lie?
The gingival zenith marks the most apical point of your gum margin on each tooth. This point determines how long your teeth appear and establishes visual symmetry.
Ideal Zenith Positions:
Maxillary central incisors: Your zenith sits slightly distal to the long axis of the tooth, approximately 1 mm toward the distal contact point
Maxillary lateral incisors: Your zenith aligns with the long axis, positioned more coronally than your central incisors
Maxillary canines: Your zenith sits distal to the long axis, positioned more apically than your central incisors
These positions create a gentle wave pattern across your anterior segment. When your dentist evaluates your smile, they check whether these zeniths align properly. Asymmetry greater than 1 mm between contralateral teeth becomes noticeable to casual observers and reduces perceived attractiveness (Chu et al., 2009).
Your gum peaks should form a wave pattern, center teeth slightly distal, side teeth centered, canines most apical and distal. This creates natural-looking symmetry.
How Should Your Gingival Contour Line Flow?
The gingival line connects the zeniths of your anterior teeth. This line should parallel your upper lip during smiling while following specific vertical relationships:
Your central incisors and canines share the same gingival line position
Your lateral incisors sit approximately 0.5-1 mm coronal to this line
This creates a gentle "gull-wing" appearance that frames your teeth elegantly
When this contour becomes flat or reversed, your smile loses dimensionality. Flat lines make teeth appear uniform and artificial. Reversed contours (laterals more apical than centrals) create an inverted smile appearance that looks pathological (Rufenacht, 1990).
What Role Does the Interdental Papilla Play in Your Smile?
The interdental papilla fills the space between your teeth below their contact points. These pink triangles complete your smile architecture and prevent unattractive "black triangles."
Your papilla height depends on two critical measurements:
Distance from bone crest to contact point: When this distance measures 5 mm or less, your papilla fills the space completely. When it exceeds 7 mm, you likely develop a black triangle (Tarnow et al., 1992).
Root proximity: Teeth with divergent roots support better papilla formation than teeth with parallel roots.
Papilla Height Prediction Based on Measurements
Bone to Contact Point Distance | Expected Papilla Fill | Clinical Appearance |
≤5 mm | 100% fill | Complete triangle, no black space |
6 mm | 50% fill | Partial fill, minor black triangle |
≥7 mm | 0-25% fill | Significant black triangle |
Losing papilla height creates immediate esthetic consequences. Black triangles make you appear older, as this condition associates with periodontal disease and aging. Food impaction occurs more frequently. Speech patterns may change as air escapes through these spaces.
How Much Gingival Display Looks Normal?

Your smile line category determines how much gum tissue shows when you smile:
Low smile line: You display less than 75% of your upper anterior teeth. No gingival tissue shows. This conservative display reads as serious or aging.
Medium smile line: You display 75-100% of your upper anterior teeth with minimal gingival display (0-2 mm). This represents the ideal for most adults.
High smile line: You display your full upper teeth plus more than 2 mm of gingival tissue. This "gummy smile" requires evaluation for possible correction.
Showing 0-2 mm of gum tissue when smiling looks ideal. Showing more than 3-4 mm creates a "gummy smile" that many patients want to correct.
High smile lines result from multiple factors: short upper lip, hypermobile lip muscles, vertical maxillary excess, or altered passive eruption (where teeth remain covered by bone and gum despite full eruption). Each cause requires different treatment approaches, from Botox injections for muscle hyperactivity to orthognathic surgery for skeletal discrepancies (Peck et al., 1992).
Why Do Proportions and Symmetry Matter More Than Perfection?
Your brain processes faces using symmetry detection. When evaluating smiles, you subconsciously compare left and right sides. Perfect bilateral symmetry rarely occurs naturally, but significant asymmetry distracts viewers.
Key proportional relationships:
Golden proportion: Your central incisor width to lateral incisor width should approximate a 1.618:1 ratio
Central dominance: Your central incisors should command attention through both size and gingival frame
Midline alignment: Your dental midline should align with your facial midline within 2-3 mm tolerance
Research demonstrates that viewers accept minor asymmetries but reject deviations greater than 2 mm in gingival margin positions between contralateral teeth (Kokich et al., 1999). This finding guides treatment planning, perfection matters less than harmony.
How Do Dentists Diagnose Gingival Esthetics?
Modern diagnosis combines traditional examination with digital technologies that enhance visualization and predictability.
What Does Clinical Examination Reveal?
Your periodontist or prosthodontist performs systematic evaluation including:
Periodontal assessment: They measure pocket depths, assess bleeding on probing, and evaluate tissue texture and color. They classify your biotype through visual inspection and probing transparency.
Smile analysis: They photograph your smile at rest, during speech, and at maximum smile. They evaluate lip dynamics, gingival display, and tooth exposure. They assess your smile arc, the relationship between your upper incisal edges and lower lip line.
Tooth-gingiva relationships: They measure clinical crown length, evaluate width-to-length ratios, and assess contact point positions. They check for the presence of black triangles and evaluate papilla fill.
How Does Digital Smile Design Transform Treatment Planning?
Digital Smile Design (DSD) revolutionized gingival esthetics by allowing visualization before treatment. This protocol follows specific steps:
Facial analysis: Your dentist photographs your face from multiple angles and analyzes proportions
Dental integration: They overlay dental parameters onto facial images
Gingival frame design: They manipulate gingival contours digitally to show potential outcomes
Patient collaboration: You participate in designing your ideal smile
Treatment simulation: They create virtual wax-ups showing final tooth positions and gingival architecture
DSD eliminates guesswork. You see your potential results before committing to treatment. Your dentist uses these designs to create surgical guides and restorative templates (Coachman et al., 2012).
What Role Do 3D Technologies Play?
Cone Beam Computed Tomography (CBCT) reveals bone architecture that determines gingival outcomes. Your dentist evaluates:
Bone crest positions relative to teeth
Root angulations and proximity
Implant placement possibilities
Defects requiring bone augmentation
Virtual planning software allows your dentist to simulate surgical procedures and predict soft tissue changes. They export these plans to 3D printers for surgical guide fabrication, ensuring precise execution of digital designs.
What Factors Limit or Complicate Gingival Esthetics?

Not every patient achieves ideal gingival esthetics due to biological and anatomical constraints.
Which Patient Characteristics Affect Outcomes?
Age: Your gum tissue thins and recedes with age. Blood supply decreases, slowing healing. Your smile line drops as facial muscles lose tone. These changes require modified treatment approaches for older patients.
Gender: Females typically show more gingival display than males. Esthetic ideals differ, feminine smiles favor more scalloped gingival contours while masculine smiles tolerate flatter architecture.
Facial morphology: Your underlying skeletal structure determines possible outcomes. Vertical growers face different challenges than horizontal growers. Your lip length and mobility set boundaries for correction.
Systemic health: Diabetes, smoking, and certain medications impair healing and tissue response. Your dentist must modify expectations and protocols accordingly.
How Do Dental Factors Influence Gingival Appearance?
Tooth position: Malpositioned teeth create gingival disharmony. Rotated teeth show asymmetric gingival margins. Intruded teeth appear too short; extruded teeth show excessive root length.
Restorative margins: Your dentist must place crown margins carefully. Violating biologic width causes inflammation and recession. Subgingival margins risk tissue discoloration, especially with metal-based restorations.
Contact points: Open contacts eliminate papilla support. Poorly shaped contacts fail to provide proper papilla framework. Your restorative dentist must establish proper contact position and form to maintain pink esthetics.
What Periodontal Limitations Exist?
Biotype constraints: Thin biotypes limit aggressive surgical approaches. You may not tolerate connective tissue grafting or crown lengthening without complications.
Bone levels: You cannot regenerate papilla beyond underlying bone support. When bone crests sit too far apically, black triangles persist despite surgical attempts.
Healing variability: Individual healing responses differ unpredictably. Some patients form excellent scar tissue; others develop keloid-like reactions or excessive recession.
How Can You Clinically Manage Gingival Esthetics?
Treatment ranges from conservative approaches to complex surgical interventions depending on your specific condition.
What Non-Surgical Options Exist?
Orthodontic correction: Moving teeth into proper position often resolves gingival disharmony. Extruding a tooth brings its gingival margin coronally. Rotating a tooth aligns its gingival zenith properly. Closing spaces improves papilla fill.
Restorative contouring: Your dentist can alter tooth shape to affect gingival appearance. Lengthening contact points apically reduces black triangles. Adding convexity to proximal surfaces supports papilla better.
Botox therapy: For gummy smiles caused by hypermobile upper lips, Botox injections reduce lip elevation during smiling. This non-surgical approach offers temporary improvement lasting 3-4 months.
Which Surgical Techniques Correct Gingival Defects?
Crown lengthening: Your periodontist removes excess gum tissue and sometimes bone to expose more clinical crown. This procedure treats "gummy smiles" or subgingival caries/restorative margins. They perform this through gingivectomy (soft tissue removal) or apically positioned flaps with osseous resection (Smukler & Chaibi, 1997).
Gingivectomy and gingivoplasty: These procedures reshape gum contours without bone removal. Your periodontist removes tissue to create symmetrical margins and proper zenith positions. Lasers or scalpels accomplish this with excellent results for thick biotypes.
Soft tissue grafting: When recession exposes roots, your periodontist harvests tissue from your palate or uses donor tissue to cover exposed surfaces. Connective tissue grafts thicken thin biotypes and improve root coverage. Free gingival grafts increase tissue thickness and keratinization.
Papilla reconstruction: Various surgical techniques attempt to regenerate lost papilla. These include pedicle flaps, semilunar coronally repositioned flaps, and injectable fillers. Success rates vary, with complete fill most predictable when initial tissue loss remains minimal (Azzi et al., 1998).
How Does Periodontal Plastic Surgery Enhance Smiles?
Periodontal plastic surgery encompasses procedures that modify gingival form for esthetics rather than health. These include:
Esthetic crown lengthening: Creating ideal gingival architecture for smile enhancement
Ridge augmentation: Building up deficient gum and bone contours before implant placement
Vestibuloplasty: Deepening the oral vestibule to allow proper tooth eruption or implant positioning
Frenectomy: Removing excessive frenum attachments that pull on gingival margins
These procedures require advanced surgical training and artistic sensibility. Your periodontist must understand both biological principles and esthetic ideals.
How Do Digital and Guided Surgeries Improve Outcomes?
Computer-guided surgery transfers digital plans to clinical reality with precision. Your surgeon uses 3D-printed guides to position osteotomy cuts exactly where planned. This accuracy proves especially valuable for:
Implant placement: Positioning fixtures to support ideal gingival contours
Crown lengthening: Resecting bone to precise levels determined preoperatively
Soft tissue grafting: Creating recipient sites that match digital designs
Studies demonstrate that guided surgery reduces operative time and improves accuracy compared to freehand techniques. The predictability enhances both functional and esthetic outcomes (Schneider et al., 2019).
Why Does Interdisciplinary Collaboration Produce Better Results?
Gingival esthetics rarely falls within a single dental specialty. Optimal outcomes require teamwork.
How Do Periodontists Contribute?
Periodontists manage the foundation. They ensure health through disease control. They perform surgical procedures that create or correct gingival architecture. They manage tissue biotypes through grafting procedures. They maintain results through ongoing maintenance care.
What Role Do Prosthodontists Play?
Prosthodontists design the final restorations that interact with gingival tissues. They determine margin placement, contact point position, and emergence profile. They create restorations that support rather than damage gingival esthetics. They coordinate the overall treatment sequence.
How Do Orthodontists Enable Gingival Harmony?
Orthodontists move teeth into positions that support ideal gingival architecture. They extrude or intrude teeth to correct gingival levels. They close spaces to improve papilla fill. They align teeth to create symmetrical gingival contours.
What Does Successful Collaboration Look Like?
Your treatment team meets before initiating care to establish shared goals. They sequence procedures logically, health before esthetics, foundation before restoration. They communicate throughout treatment, adjusting plans as tissue response dictates. They share responsibility for final outcomes.
This collaboration proves essential for complex cases involving multiple missing teeth, severe malposition, or significant tissue loss. No single specialist can address all aspects optimally (Spear et al., 2008).
What Challenges and Limitations Should You Understand?

Despite advances, gingival esthetics faces inherent constraints.
Why Does Esthetic Perception Vary?
Beauty standards differ across cultures and individuals. What appears ideal to your dentist may not match your preferences. Some patients prefer flat gingival lines; others want pronounced scalloping. Cultural backgrounds influence acceptable gingival display.
Research shows that laypeople tolerate greater deviations from ideal parameters than dentists do. Your perception of your own smile differs from how others see it. These subjective factors complicate treatment planning and satisfaction assessment.
What Biological Constraints Exist?
Your tissue biotype limits surgical options. Your healing response affects outcomes. Your bone architecture determines possible papilla fill. These biological realities prevent achieving identical results across all patients.
Relapse occurs. Gingival margins creep apically over time. Papilla shrinks as tissue matures. These changes require maintenance and sometimes retreatment.
How Do Technical Limitations Affect Results?
Surgical skill varies. Not all clinicians achieve identical outcomes with the same techniques. Digital planning requires expensive technology and training. Guided surgery adds cost and complexity.
Some defects resist complete correction. Severe tissue loss, significant asymmetry, or unfavorable biotypes may yield improvement rather than perfection.
What Future Innovations Will Transform Gingival Esthetics?
Emerging technologies promise to enhance predictability and outcomes.
How Will Artificial Intelligence Personalize Smile Design?
AI algorithms analyze thousands of successful smiles to identify patterns that predict patient satisfaction. Machine learning helps dentists select ideal gingival parameters based on your facial features and preferences. Predictive modeling shows how your tissues will age and heal, allowing proactive treatment planning.
Computer vision systems evaluate your smile automatically, identifying deviations from ideal parameters more objectively than human assessment. These tools augment clinical judgment rather than replacing it.
What Minimally Invasive Techniques Are Emerging?
Laser dentistry: Soft tissue lasers allow precise gingival contouring with minimal bleeding and faster healing. They disinfect as they cut, reducing postoperative infection risk. They create smooth tissue surfaces that heal with less scarring.
Microsurgical approaches: Operating microscopes and miniature instruments enable procedures through smaller incisions. Microsutures (as small as 8-0) approximate tissue with minimal trauma. These techniques improve healing and reduce patient discomfort.
Biological mediators: Growth factors, stem cells, and tissue engineering products enhance healing and tissue regeneration. Platelet-rich fibrin (PRF) accelerates soft tissue healing. Enamel matrix derivatives improve periodontal regeneration. These biologics expand treatment possibilities.
Injectable fillers: Hyaluronic acid fillers offer temporary papilla augmentation without surgery. They fill black triangles immediately, though results last only months. Future bioactive fillers may stimulate natural tissue regeneration.
Conclusion: What Should You Remember About Gingival Esthetics?
Gingival esthetics has evolved from an afterthought to a central component of smile design. Your gums frame your teeth and significantly impact your overall facial appearance. Understanding the key parameters, gingival zenith, contour, papilla fill, and display, helps you evaluate your own smile and communicate with your dental team.
Modern diagnosis combines clinical examination with digital technologies that enhance visualization and predictability. Treatment ranges from simple orthodontic movement to complex periodontal surgery depending on your specific needs. Success requires interdisciplinary collaboration and realistic expectations about biological limitations.
The future promises AI-assisted design, minimally invasive techniques, and biological enhancements that will make optimal gingival esthetics more achievable for more patients. However, the fundamental principles remain constant: health precedes beauty, biology dictates possibility, and individual variation requires personalized approaches.
Your journey toward ideal gingival esthetics begins with consultation with qualified specialists who understand these principles. Through proper diagnosis, careful planning, and skilled execution, you can achieve a smile where pink and white esthetics work in harmony to create natural, attractive results.
References
Azzi, Roberto, et al. "Root coverage and papilla reconstruction using autogenous osseous and connective tissue grafts." International Journal of Periodontics & Restorative Dentistry, vol. 18, no. 5, 1998, pp. 455-463.
Chu, Stephen J. "Range of gingival display in normal smiling: The ideal range of gingival display." Journal of Prosthetic Dentistry, vol. 97, no. 5, 2007, pp. 259-260.
Chu, Stephen J., et al. "The gingival zenith position: A clinical and biometric evaluation." Journal of Prosthetic Dentistry, vol. 101, no. 1, 2009, pp. 48-55.
Coachman, Christian, et al. "Digital Smile Design: A tool for treatment planning and communication in esthetic dentistry." Quintessence of Dental Technology, vol. 35, 2012, pp. 1-8.
Gargiulo, Angelo W., et al. "Dimensions and relations of the dentogingival junction in humans." Journal of Periodontology, vol. 32, no. 3, 1961, pp. 261-267.
Kokich, Vincent O., et al. "Comparing the perception of dentists and lay people to altered dental esthetics." Journal of Esthetic and Restorative Dentistry, vol. 11, no. 6, 1999, pp. 311-324.
Lang, Niklaus P., and Peter M. Bartold. "Periodontal health." Journal of Clinical Periodontology, vol. 45, no. 20, 2018, pp. S9-S16.
Müller, Hans-Peter, et al. "Thin gingival biotype." Journal of Clinical Periodontology, vol. 27, no. 1, 2000, pp. 1-8.
Newman, Michael G., et al. Carranza's Clinical Periodontology. 12th ed., Elsevier Saunders, 2015.
Peck, Sheldon, et al. "The gingival smile line." Angle Orthodontist, vol. 62, no. 2, 1992, pp. 91-100.
Rufenacht, Claude R. Fundamentals of Esthetics. Quintessence Publishing, 1990.
Schneider, David, et al. "Guided bone regeneration with simultaneous implant placement: Clinical and radiographic outcomes." Clinical Oral Implants Research, vol. 30, no. 5, 2019, pp. 414-424.
Seibert, John S., and Jan Lindhe. "Esthetics and periodontal therapy." Textbook of Clinical Periodontology, edited by Jan Lindhe, Munksgaard, 1989, pp. 477-514.
Smukler, Henry, and Mohammed Chaibi. "Periodontal and dental considerations in clinical crown extension: A rational basis for treatment." International Journal of Periodontics & Restorative Dentistry, vol. 17, no. 5, 1997, pp. 464-477.
Spear, Frank M., et al. "Interdisciplinary management of single-tooth implants." Seminars in Orthodontics, vol. 14, no. 4, 2008, pp. 234-248.
Tarnow, Dennis P., et al. "The effect of the distance from the contact point to the crest of bone on the presence or absence of the interproximal dental papilla." Journal of Periodontology, vol. 63, no. 12, 1992, pp. 995-996.



