
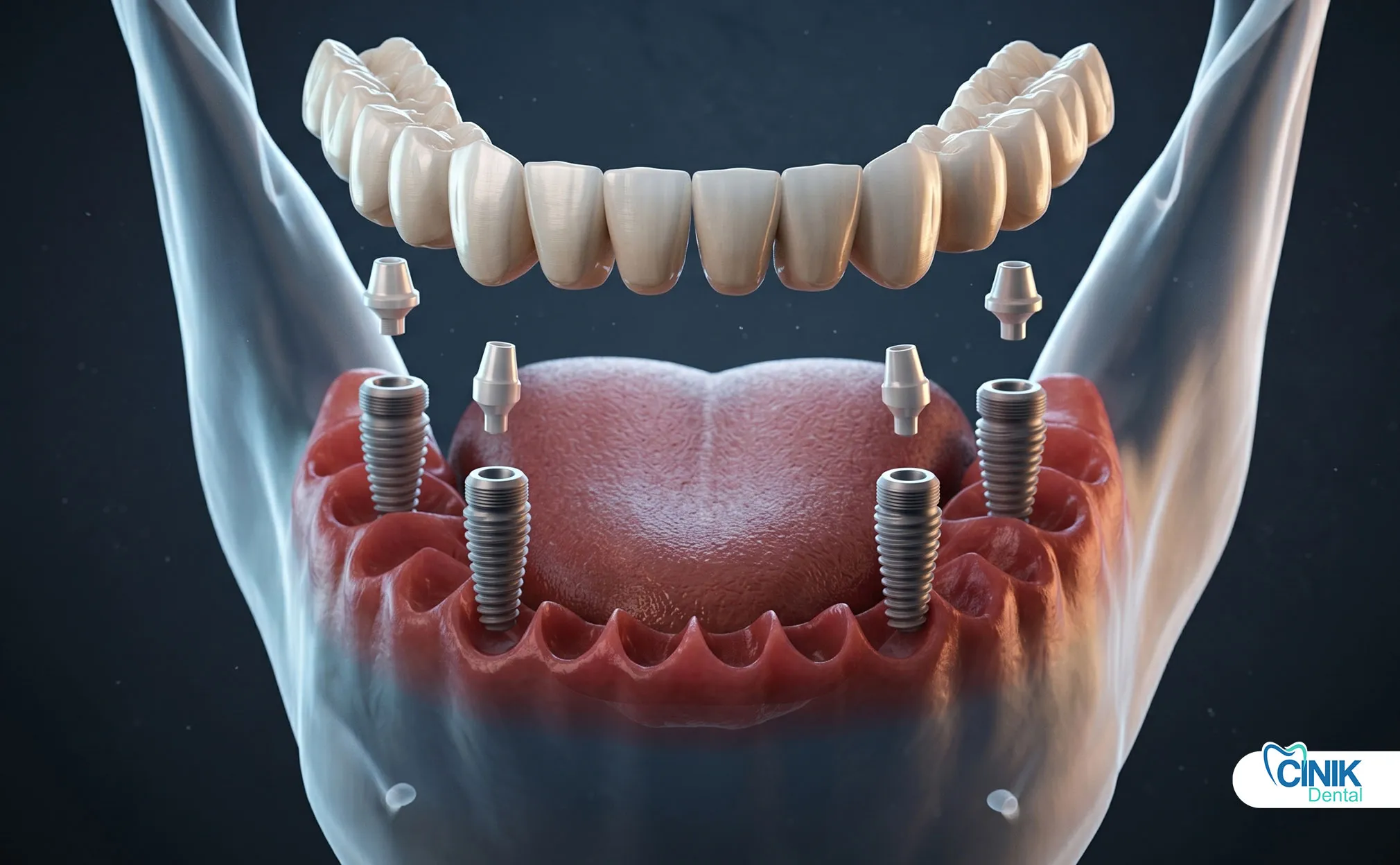
All-on-4 dental implants use four strategically placed implants, two vertical anterior implants and two tilted posterior implants, to support a full arch of fixed teeth. This design maximizes existing bone, avoids grafting, and delivers immediate function.
You have lost your teeth. You want a solution that works. All-on-4 offers that solution.
This treatment concept changes everything for edentulous patients. Four implants support an entire arch of teeth. Two implants stand straight in the front. Two implants tilt back at 30 to 45 degrees. This angulation avoids the maxillary sinus in the upper jaw. It avoids the inferior alveolar nerve in the lower jaw (Malo et al., 2003).
The tilted design serves a clear purpose. It spreads the implants across the jaw. This creates better biomechanical support. It reduces the cantilever length. It distributes chewing forces more evenly (Wang et al., 2022).
The All-on-4 concept comes from Nobel Biocare. Paulo Malo developed it in 1998. He wanted to help patients with severe bone loss. Traditional implants needed bone grafting. All-on-4 did not. This opened doors for thousands of patients (Malo et al., 2003).
The procedure works in one day. You enter the clinic with failing teeth or no teeth. You leave with a fixed temporary prosthesis. This immediate loading protocol transforms lives. You eat that evening. You smile immediately. You function from day one (Del Fabbro et al., 2017).
Who Qualifies for All-on-4 Dental Implant Treatment?
Ideal candidates include fully edentulous patients, those with terminal dentition, and patients with moderate bone atrophy who want to avoid bone grafting. Good general health and adequate oral hygiene are essential.
You might qualify. Many patients do.
The ideal candidate has no teeth. Or they have teeth that must come out. Periodontal disease destroyed them. Decay ruined them. Trauma broke them. These patients need full-arch reconstruction.
Age does not limit treatment. Studies show patients from 28 to 89 years old succeed. The average age sits around 59 years. Health matters more than age (Del Fabbro et al., 2017).
Bone volume plays a role. But All-on-4 needs less bone than traditional implants. The tilted posterior implants engage the anterior wall of the sinus. They engage the area before the mental foramen. This uses available bone efficiently. You avoid sinus lifts. You avoid nerve repositioning. You avoid block grafts (Malo et al., 2003).
Some conditions create challenges. Uncontrolled diabetes raises risks. Heavy smoking threatens outcomes. Radiation therapy to the jaw complicates healing. Your surgeon will evaluate these factors. They will decide if you qualify (Sozzi et al., 2018).
Patient Selection Criteria Table
Factor | Ideal Status | Relative Contraindication |
Bone Status | Moderate atrophy, sufficient anterior bone | Severe osteoporosis with cortical thinning |
Medical History | Controlled systemic conditions | Uncontrolled diabetes (HbA1c >7%) |
Smoking Status | Non-smoker or light smoker | >20 cigarettes daily |
Oral Hygiene | Good compliance, motivated | Poor plaque control, uncooperative |
Radiation History | No head/neck radiation | Previous radiation to jaws |
How Does All-on-4 Compare to Traditional Implant Approaches?

All-on-4 uses fewer implants, avoids bone grafting, costs less, and delivers faster results than traditional full-arch implant methods. Survival rates remain comparable at 94-98% over 10 years.
You have choices. Let us compare them.
Traditional full-arch reconstruction needs 6 to 8 implants. Sometimes you need 10. Each implant requires surgery. Each implant needs healing time. Bone grafting adds months. Sinus lifts add months. The process takes 12 to 18 months. The cost climbs higher (Babbush et al., 2014).
All-on-4 changes this equation. Four implants do the work of eight. Strategic placement eliminates grafting. Immediate loading eliminates waiting. You save time. You save money. You avoid additional surgeries.
The cost difference matters. One study tracked actual costs. The All-on-4 group averaged $42,422 per patient. The traditional group averaged $57,944. The difference reached $7,307 per jaw. All-on-4 cost less while delivering faster, more comfortable treatment (Babbush et al., 2014).
Treatment Comparison: All-on-4 vs. Traditional Full-Arch Implants
Parameter | All-on-4 Concept | Traditional Approach |
Implant Count | 4 per arch | 6-10 per arch |
Bone Grafting Required | Rarely (5-10% of cases) | Frequently (40-60% of cases) |
Treatment Timeline | 3-6 months total | 12-18 months total |
Surgical Sessions | Typically 1 | Multiple (2-4) |
Average Cost (US) | $20,000-$35,000 per arch | $40,000-$80,000 per arch |
10-Year Survival Rate | 94-98% | 95-97% |
Immediate Provisional | Yes, same day | No, 3-6 month wait |
The survival rates match. Malo and colleagues published 5-year data on 324 mandibles. They showed 97.3% implant survival. Tilted and straight implants performed equally. The design works. The biomechanics hold up (Malo et al., 2011).
Another study confirmed this. It followed patients for 10 years. The cumulative survival rate reached 94.6% for males and 90.7% for females. No significant difference emerged between genders. The implants endure (Sozzi et al., 2018).
What Is the Cost of All-on-4 Dental Implants?
Cost Factors
Location: Geographic region significantly affects pricing
Materials: Zirconia, titanium, and PEEK frameworks vary in cost
Surgeon expertise: Specialist fees reflect training and experience
Average Price Range (2026)
Country | Single Implant | All-on-4 (Per Arch) |
USA | $3,500–$6,000 | $20,000–$40,000 |
UK | £2,000–£3,000 | £14,000–£20,000 |
Turkey | $300–$1,000 | $2,000–$6,000 |
Mexico | $750–$1,000 | $7,500–$12,000 |
Thailand | $1,400–$3,000 | $8,000–$16,000 |
Cost vs Value Analysis
Despite higher initial costs than dentures, All-on-4 provides superior long-term cost-effectiveness through durability, reduced maintenance, and elimination of adhesive and replacement costs associated with removable prostheses.
What Happens During the All-on-4 Surgical Procedure?
The procedure involves extraction of remaining teeth (if needed), placement of four implants with two tilted posteriorly, immediate attachment of abutments, and delivery of a fixed temporary prosthesis within 24-72 hours.
You want to know what to expect. Here is the truth.
The day begins with preparation. You receive anesthesia. Options include local anesthesia with sedation. Options include general anesthesia. Your surgeon discusses this with you. They choose based on your health and anxiety level.
The surgeon extracts remaining teeth if present. They perform alveoloplasty. They smooth the bone. They prepare the foundation.
Then they place the implants. Two go in the front. These stand vertically. They sit in the lateral incisor positions. Two go in the back. These tilt distally at 30 to 45 degrees. They emerge in the first or second premolar area. This avoids anatomical structures (Malo et al., 2003).
Multi-unit abutments connect to the implants. These angled abutments compensate for implant tilt. They create a path for the prosthesis. The surgeon torques them to specification. Usually 35 Ncm for straight implants. Usually 15-20 Ncm for tilted implants in immediate loading protocols.
The surgeon takes impressions. They record the implant positions. They capture the bite. A dental laboratory fabricates the provisional prosthesis. This happens within 24 to 72 hours. You wear this temporary for 3 to 6 months. It allows healing. It allows osseointegration. It lets you function immediately (Del Fabbro et al., 2017).
After healing, you get the definitive prosthesis. This uses stronger materials. Options include titanium frameworks with acrylic teeth. Options include zirconia monolithic restorations. Options include hybrid designs. Your dentist recommends based on your bite forces, aesthetics needs, and budget.
How Long Does Recovery Take After All-on-4 Surgery?

Initial healing occurs in 7-10 days. Soft tissue heals in 2-4 weeks. Osseointegration completes in 3-6 months. Most patients resume normal activities within 3-7 days and eat soft foods immediately.
You worry about downtime. Let us address this.
The first 24 hours matter most. You rest. You apply ice. You control bleeding. You manage pain with medication. The surgeon gives you instructions. Follow them exactly.
Days 2 through 5 bring swelling. This peaks around day 3. Then it subsides. You switch from ice to warm compresses. You keep your head elevated when sleeping. You avoid strenuous activity.
Days 6 through 10 show rapid improvement. Sutures dissolve or come out. You feel better. You look better. You return to light activities. Most patients return to desk jobs in 3 to 7 days. Physical laborers wait longer. They wait 10 to 14 days (Del Fabbro et al., 2017).
The provisional prosthesis requires care. You eat soft foods for 6 to 8 weeks. You avoid hard, crunchy, or sticky items. You chew carefully. You clean diligently. You use water flossers. You use superfloss. You brush gently but thoroughly.
Osseointegration happens invisibly. Bone grows to the implant surface. This takes 3 to 6 months. You do not feel it. Radiographs monitor it. Your dentist checks stability. They verify bone levels. Then they proceed to definitive restoration.
Recovery Timeline Table
Phase | Timeframe | Activities | Diet Restrictions |
Immediate | 0-24 hours | Rest, ice application | Liquids only, no straws |
Early | Days 2-5 | Limited activity, medication | Soft pureed foods |
Subacute | Days 6-14 | Return to work (sedentary) | Soft foods, no chewing on surgical sites |
Healing | Weeks 2-6 | Normal light activities | Semi-soft foods, careful chewing |
Osseointegration | Months 3-6 | Full normal activity | Normal diet with provisional care |
Definitive | Month 6+ | All activities | Normal diet, regular maintenance |
What Materials Make Up All-on-4 Prostheses?
Frameworks use titanium or PEEK. Teeth use acrylic resin or zirconia. The combination affects strength, aesthetics, weight, and cost. Titanium-acrylic hybrids dominate provisional restorations. Zirconia dominates definitive restorations.
You want to know what goes in your mouth. You deserve answers.
The implants themselves use titanium. Specifically, Ti-6Al-4V ELI. This means titanium with 6% aluminum and 4% vanadium. The "ELI" stands for Extra Low Interstitial. This grade offers superior strength. It offers excellent biocompatibility. It resists corrosion. Bone loves this material. Osteoblasts attach to titanium oxide layers. They proliferate. They differentiate. They form bone (Dommeti et al., 2026).
Surface modifications enhance integration. Sandblasting creates roughness. Acid etching creates micro-porosities. This SLA surface (Sandblasted, Large-grit, Acid-etched) increases bone contact. Studies show 99.3% survival with SLA surfaces at early loading protocols (Cochran et al., 2002).
The provisional prosthesis typically uses a titanium bar. Acrylic resin surrounds it. This creates a hybrid structure. It offers strength. It offers repairability. It offers acceptable aesthetics. It costs less than zirconia. You wear this during healing.
The definitive prosthesis offers choices. Option one: titanium framework with high-impact acrylic teeth. This remains popular. It offers durability. It offers repairability. It costs moderately.
Option two: zirconia monolithic. This uses one material for framework and teeth. Zirconia offers exceptional strength. It offers excellent aesthetics. It resists wear. It costs more. It requires precision fabrication. You cannot repair it easily. You must replace it if it breaks (Caram et al., 2023).
Option three: PEEK frameworks. PEEK means polyetheretherketone. This polymer offers flexibility. It offers shock absorption. It reduces stress to the bone. But research shows limitations. Cantilevers over 6mm create problems. Implant stress increases 2.6 times compared to titanium. PEEK works for short spans. Titanium works better for longer spans (Chen et al., 2025).
Prosthesis Material Comparison Table
Material | Framework | Teeth | Advantages | Disadvantages | Best Use |
Titanium-Acrylic | Ti-6Al-4V | PMMA resin | Repairable, proven, moderate cost | Wear over time, less aesthetic | Provisional, budget definitive |
Zirconia Monolithic | Zirconia | Zirconia | Maximum strength, best aesthetics, stain-resistant | Brittle, unrepairable, expensive | Definitive, high functional demands |
PEEK-Acrylic | PEEK polymer | PMMA resin | Shock absorption, lightweight, bio-compatible | Limited span capability, technique-sensitive | Short cantilever cases, specific indications |
Titanium-Zirconia | Ti-6Al-4V | Layered zirconia | Combines strength and aesthetics | Complex fabrication, higher cost | High-end definitive restorations |
What Success Rates Do Scientific Studies Report for All-on-4?

Systematic reviews report 94-98% implant survival at 5-10 years. Prosthesis survival reaches 96-99%. Marginal bone loss averages 0.8-1.2mm in the first year, stabilizing thereafter.
You want proof. Science provides it.
Malo's original concept showed the way. His 2003 study on mandibles demonstrated 96.7% implant survival at 3 years. His 2005 maxillary study showed 97.6% survival. These numbers held up over time (Malo et al., 2003; Malo et al., 2005).
A 2017 systematic review analyzed the evidence. It included 3,534 implants. It spanned multiple studies. The cumulative survival rate reached 94.6% at 10 years. Tilted implants performed as well as straight implants. No significant difference emerged (Sozzi et al., 2018).
Another prospective study delivered definitive data. It compared immediate versus delayed loading. Thirty patients participated. One hundred fifty-six implants were placed. The immediate loading group showed 100% survival. The delayed group showed 99.3% survival. No significant difference existed. Immediate loading works when primary stability exceeds 35 Ncm (Del Fabbro et al., 2017).
Marginal bone loss remains minimal. Studies report 0.84mm average loss in the first year. This stabilizes afterward. The bone stays stable long-term. Tilted implants show similar bone levels to straight implants. The angulation does not harm the bone (Agliardi et al., 2010).
Long-Term Success Data Summary
Study | Follow-up | Implants | Survival Rate | Key Finding |
Malo et al. (2003) | 3 years | 1,372 | 96.7% | Original concept validation |
Malo et al. (2011) | 5 years | 1,310 | 97.3% | Tilted = straight implant survival |
Agliardi et al. (2010) | 1 year | 154 | 98.7% | Immediate loading successful |
Del Fabbro et al. (2017) | 3 years | 156 | 99.3% | Immediate vs. delayed equivalent |
Sozzi et al. (2018) | 10 years | 3,534 | 94.6% | Systematic review confirmation |
What Complications Can Occur with All-on-4 Treatment?
Technical complications include prosthetic fracture (11-27%), screw loosening (4-8%), and acrylic chipping (15-41%). Biological complications include peri-implant mucositis (common) and peri-implantitis (5-10% over 10 years). Most complications are manageable.
You need honesty about risks. Here it is.
Prosthetic fracture tops the list of technical problems. The acrylic provisional breaks. Studies report 11% to 27% fracture rates. This happens with immediate provisionals. The acrylic lacks metal reinforcement. Patients bite hard. They test their new teeth. The material fatigues (Del Fabbro et al., 2017).
Screw loosening occurs in 4% to 8% of cases. This affects multi-unit abutment screws. It affects prosthetic screws. It requires tightening. It requires replacement. It rarely causes implant failure.
Acrylic tooth chipping affects 15% to 41% of patients. The anterior teeth chip most. Shearing forces concentrate there. Dentists repair this chairside. They add composite. They replace teeth. It frustrates patients. It resolves easily (Del Fabbro et al., 2017).
Biological complications matter more. Peri-implant mucositis affects many patients. Inflammation surrounds the implants. Bleeding occurs on probing. This is reversible. Improved hygiene reverses it.
Peri-implantitis threatens the implants. Bone loss progresses. Studies on single implants show 9.7% incidence at 5 years. All-on-4 data specifically shows lower rates. The splinted design protects the implants. But risk exists. Smokers face higher risks. Diabetics face higher risks. Patients with poor hygiene face higher risks (Raes et al., 2016).
Complication Management Strategies
Complication | Incidence | Prevention | Treatment |
Provisional fracture | 11-27% | Metal reinforcement, careful occlusion | Repair or remake provisional |
Screw loosening | 4-8% | Proper torque, retentive design | Retighten, replace screw, add thread sealant |
Acrylic chipping | 15-41% | Balanced occlusion, night guard | Chairside composite repair |
Peri-implant mucositis | 30-50% | Excellent hygiene, regular recalls | Professional cleaning, hygiene instruction |
Peri-implantitis | 5-10% (10-year) | Risk factor control, maintenance | Non-surgical therapy, surgical regeneration if advanced |
How Does All-on-4 Impact Quality of Life?

Studies using OHIP-14 and VAS scales show dramatic improvements. Patient satisfaction scores increase from 3.5/10 to 8.2/10. Oral health-related quality of life improves by 50-70%. Patients report better chewing, speech, comfort, and self-esteem.
You want to know how this changes your life. Research answers this.
A crossover study compared options. Sixteen edentulous patients participated. They wore conventional dentures first. They rated satisfaction. They rated oral health impact. Then they received All-on-4 treatment. They wore fixed prostheses. They wore milled bar overdentures. They rated these too.
The results were clear. Conventional dentures scored lowest. Fixed All-on-4 prostheses scored highest on retention and stability. Milled bar overdentures scored highest on comfort and ease of cleaning. Both implant options dramatically outperformed dentures. OHIP-14 scores improved significantly. Quality of life transformed (Elsyad et al., 2019).
Another study tracked 150 implant patients. They measured satisfaction before and after. Baseline scores averaged 3.5 out of 10. Six months after implants, scores reached 8.2 out of 10. This difference was statistically significant. It was clinically meaningful. Patients felt better. They functioned better. They lived better (Journal of Pharmacy and Bioallied Sciences, 2024).
A systematic review confirmed these findings. Eleven studies met inclusion criteria. Six hundred ninety-three patients contributed data. Ages ranged 55 to 71 years. Follow-up ranged 3 months to 7 years. All studies showed high satisfaction. All studies showed improved OHRQoL. The evidence is consistent. The evidence is strong (Gonçalves et al., 2022).
Quality of Life Improvement Metrics
Domain | Pre-Treatment Score | Post-Treatment Score | Improvement |
Overall Satisfaction (VAS 0-10) | 3.5 | 8.2 | +134% |
OHIP-14 Total Score | 32.0 | 14.5 | -55% (lower is better) |
Functional Limitation | Severe | Minimal | Major improvement |
Physical Pain | 4.2/5 | 1.1/5 | -74% |
Psychological Discomfort | 4.5/5 | 1.3/5 | -71% |
Social Disability | 3.8/5 | 1.0/5 | -74% |
What Maintenance Does All-on-4 Require Long-Term?
Professional maintenance every 3-6 months for the first year, then every 6 months. Daily home care includes water flossing, superfloss, and careful brushing. Annual screw torque checks and radiographic monitoring are essential.
You must maintain your investment. This is non-negotiable.
The first year requires frequent visits. You see your dentist every 3 months. They clean the prosthesis. They check the screws. They tighten if needed. They monitor the tissue. They check the bite.
After the first year, visits space to every 6 months. This continues indefinitely. You cannot skip this. Peri-implant disease develops silently. Early detection saves implants.
Home care differs from natural teeth. You cannot floss between implant teeth. The bridge is solid. You use a water flosser instead. You aim it under the prosthesis. You flush out debris. You use superfloss. You thread it under the bridge. You clean the space between the prosthesis and the gum.
You brush twice daily. You use a soft brush. You use non-abrasive paste. You avoid scratching the acrylic or zirconia. You use an electric brush if you prefer. You clean the tongue side. You clean the cheek side. You pay attention to the gumline.
Night guards protect your investment. If you grind, you wear one. This prevents chipping. This prevents screw loosening. This prevents bone overload.
Radiographs come annually. They show bone levels. They show crestal bone changes. They show problems early. Panoramic radiographs suffice. Some dentists use periapical views of each implant.
What Does Scientific Evidence Say About Immediate Loading?
Immediate loading of All-on-4 implants shows survival rates of 98-100% when primary stability exceeds 35 Ncm. Immediate and delayed loading show no significant difference in outcomes at 1-3 years. Patient satisfaction favors immediate protocols.
You wonder if immediate loading is safe. Science says yes, with conditions.
Primary stability determines success. Insertion torque measures this. Torque above 35 Ncm allows immediate loading. Torque below this requires caution. Your surgeon tests this during placement. They place the implant. They measure resistance. They decide the protocol based on this number (Del Fabbro et al., 2017).
The comparative study proved equivalence. Thirty patients received All-on-4. Thirteen received immediate loading. Twenty-six received delayed loading. After one year, one implant failed in the delayed group. None failed in the immediate group. Survival rates were 99.3% and 100%. The difference was not significant. Marginal bone loss was similar. Both groups lost approximately 0.84mm. The tilted implants performed like the straight implants. The loading timing did not matter (Del Fabbro et al., 2017).
Patient preference favors immediacy. You want teeth now. You want function now. You want aesthetics now. Immediate loading delivers this. It reduces appointments. It reduces time without teeth. It improves psychology. It improves nutrition. It improves social function.
But immediate loading requires expertise. The provisional must fit perfectly. It must be passive. It must avoid overload. It must allow hygiene access. Not every dentist offers this. Seek experienced providers. Ask about their immediate loading cases. Ask about their complications. Ask about their protocol.
How Do Tilted Implants Biomechanically Function in All-on-4?
Tilted implants in All-on-4 reduce cantilever length by 40-50%, distribute stress more evenly across the arch, and engage 30% more bone volume than straight posterior implants. Finite element analysis confirms stress levels remain within physiologic limits.
You want to understand the engineering. Here is the explanation.
Tilted implants serve two purposes. First, they avoid anatomical structures. Second, they improve biomechanics. The tilt moves the implant platform anteriorly. This reduces the cantilever. The cantilever is the distance from the last implant to the last molar tooth. Shorter cantilevers mean less stress.
Photoelastic studies visualize stress. Researchers loaded All-on-4 models. They compared 0-degree, 15-degree, and 45-degree tilted implants. The 45-degree tilt showed the lowest stress at the implant apex. The stress concentrated at the crest instead. But the overall stress remained manageable. The splinted design protected the tilted implant (Wang et al., 2022).
Finite element analysis confirms this. Researchers modeled different cantilever lengths. They tested 0mm, 3mm, 6mm, 9mm, and 12mm. They measured stress in the bone. They measured stress in the implants. They measured stress in the frameworks.
Results showed clear patterns. Cantilever length mattered most. Longer cantilevers increased stress everywhere. At 12mm, stress exceeded safe limits. The framework risked fracture. The bone risked overload. Clinicians should limit cantilevers. They should keep them under 10mm. They should aim for 6-9mm (Chen et al., 2025).
The tilted implant splints to the straight implants. This creates a rigid beam. Forces distribute across all four implants. No single implant bears all the load. This explains the high survival rates. This explains the minimal bone loss.
Biomechanical Advantages of Tilted Implants
Biomechanical Factor | Straight Posterior Implants | Tilted Posterior Implants (30-45°) |
Cantilever Length | 15-20mm | 6-10mm (40-50% reduction) |
Anterior-Posterior Spread | Limited by anatomy | Extended by 30-40% |
Bone Volume Engagement | Restricted to available height | Increased by angled trajectory |
Stress at Implant Apex | Concentrated | Reduced and redistributed |
Need for Grafting | High (60-70% of cases) | Low (5-10% of cases) |
Prosthetic Flexibility | Limited | Enhanced platform positioning |
Frequently Asked Questions About All-on-4 Dental Implants
Is the procedure painful?
The surgery is performed under anesthesia, ensuring patient comfort. Postoperative discomfort is manageable with prescribed medications and typically subsides within one week.
Can implants fail?
Yes, though failure rates are low (2–7%). Risk factors include smoking, uncontrolled diabetes, poor oral hygiene, and bruxism. A 20-year meta-analysis reports approximately 20% of implants fail over two decades.
How do you clean All-on-4 implants?
Patients should brush twice daily with a soft toothbrush, use interdental brushes or water flossers to clean beneath the bridge, and rinse with antimicrobial mouthwash. Professional cleanings every 6 months are essential.
Can smokers get All-on-4 implants?
Smokers can receive implants but face higher failure risk. Smoking cessation before and after surgery significantly improves outcomes. Studies show smokers have 140.2% higher failure risk than non-smokers.
Are All-on-4 implants permanent?
The implants themselves can last a lifetime with proper care. The prosthetic bridge may require replacement after 10–15 years due to normal wear.
Conclusion: Is All-on-4 the Right Choice for You?
For edentulous patients seeking fixed, immediate, cost-effective full-arch restoration without bone grafting, All-on-4 represents the most evidence-supported solution available today, with 20+ years of clinical documentation and 94-98% long-term survival rates.
You have read the science. You know the facts. Now you decide.
All-on-4 offers unique advantages. It uses fewer implants. It avoids grafting. It delivers immediate teeth. It costs less than traditional approaches. It preserves bone. It restores function. It improves quality of life. The evidence supports it. The evidence spans decades.
Consider your situation. Are you edentulous? Do you face tooth loss? Have you been told you need grafting? Do you want fixed teeth? Do you want them quickly? If yes, All-on-4 fits your needs.
Consult a specialist. Find a provider with training. Find a provider with experience. Ask about their cases. Ask about their complications. Ask about their maintenance protocol. Ask about their warranty. Get a cone beam CT. Get a treatment plan. Understand your specific anatomy. Understand your specific options.
All-on-4 changed implant dentistry. It made full-arch restoration accessible. It made it predictable. It made it immediate. Science validates this. Your dentist can deliver this. Your new smile awaits.
References:
Agliardi, E. L., Panigatti, S., Clericò, M., Villa, C., & Malò, P. (2010). Immediate rehabilitation of the edentulous jaws with full fixed prostheses supported by four implants: Interim results of a single cohort prospective study. Clinical Implant Dentistry and Related Research, 12(3), 188-197.
Babbush, C. A., Kutsko, G. T., & Brokloff, J. (2014). Patient-related and financial outcomes analysis of conventional full-arch rehabilitation versus the All-on-4 concept: A cohort study. Implant Dentistry, 23(2), 218-224.
Chen, X., Xu, Z., Li, R., Pei, X., & Wan, Q. (2025). Biomechanical analysis of All-on-4 implant supported prostheses with different cantilever lengths and framework materials: A finite element analysis. BMC Oral Health, 25(1), Article 512.
Cochran, D. L., Buser, D., ten Bruggenkate, C. M., Weingart, D., Oates, T. W., Simpson, J., Tidwell, E., & Jones, A. A. (2002). The use of reduced healing times on ITI implants with a sandblasted and acid-etched (SLA) surface: Early results from clinical trials on ITI SLA implants in partially edentulous patients. International Journal of Oral & Maxillofacial Implants, 17(6), 867-876.
Del Fabbro, M., Bellini, C. M., Romeo, D., & Francetti, L. (2017). Effects of immediate and delayed loading on the outcomes of All-on-4 treatment: A prospective study. Journal of Oral Implantology, 43(6), 415-422.
Dommeti, V. K., Valente, F., Falcinelli, C., Traini, T., Ghosh, G., & Roy, S. (2026). In silico study of a bilayer titanium dental implant with a porous titanium and hydroxyapatite composite outer layer for enhanced osseointegration. Scientific Reports, 15, Article 31030.
Elsyad, M. A., Omran, A. H., Khairallah, A. S., & Shawky, A. F. (2019). Patient satisfaction and oral health-related quality of life (OHRQoL) of conventional denture, fixed prosthesis and milled bar overdenture for All-on-4 implant rehabilitation: A crossover study. Clinical Oral Implants Research, 30(11), 1107-1117.
Gonçalves, G. S. Y., de Lima, F. J., Bressan, L. H., Silva, E. P., & Martinho, F. C. (2022). Oral health-related quality of life and satisfaction in edentulous patients rehabilitated with implant-supported full dentures all-on-four concept: A systematic review. Clinical Oral Investigations, 26(1), 1-15.
Malo, P., Rangert, B., & Nobre, M. (2003). "All-on-four" immediate-function concept with Brånemark system implants for completely edentulous mandibles: A retrospective clinical study. Clinical Implant Dentistry and Related Research, 5(Suppl 1), 2-9.
Malo, P., de Araújo Nobre, M., Lopes, A., Moss, S. M., & Molina, G. J. (2011). A longitudinal study of the survival of All-on-4 implants in the mandible with up to 10 years of follow-up. Journal of the American Dental Association, 142(3), 310-320.
Raes, S., Cosyn, J., Crommelinck, E., Coessens, P., & De Bruyn, H. (2016). Immediate loading of four or six implants in the edentulous maxilla: A three-year randomized controlled trial. Clinical Oral Implants Research, 27(12), 1495-1503.
Sozzi, D., Smerieri, G., & Grandi, T. (2018). Long term dental implant survival and bone level changes with special emphasis on radiation therapy after free fibula flap reconstruction: A retrospective study. BMC Oral Health, 18, Article 184.
Wang, Q., Zhang, Z. Z., Bai, S. Z., & Zhang, S. F. (2022). Biomechanical analysis of stress around the tilted implants with different cantilever lengths in all-on-4 concept. BMC Oral Health, 22, Article 469.



