
What Are Wisdom Teeth and Why Do They Matter?
Wisdom teeth are the third and final set of molars that typically emerge between ages 17 and 25. They often cause problems because modern human jaws are too small to accommodate them properly.
Wisdom teeth, clinically known as third molars, represent the last teeth to develop in the human dentition. These teeth earned their common name because they appear during the "age of wisdom", late adolescence to early adulthood (Carter and Worthington, 2016). Anthropologists trace their evolutionary origins to our ancestors, who required these powerful grinding teeth to process coarse, fibrous diets. However, dietary changes and jaw size reduction over millennia have rendered wisdom teeth largely vestigial in contemporary populations (Venta et al., 2018).
Table 1: Evolutionary Context of Third Molars
Era | Diet Type | Jaw Size | Wisdom Tooth Function |
Paleolithic | Coarse, uncooked vegetation | Large, robust | Essential for grinding |
Neolithic | Mixed, partially processed | Moderate | Supplementary grinding |
Modern | Soft, processed foods | Reduced | Often non-functional |
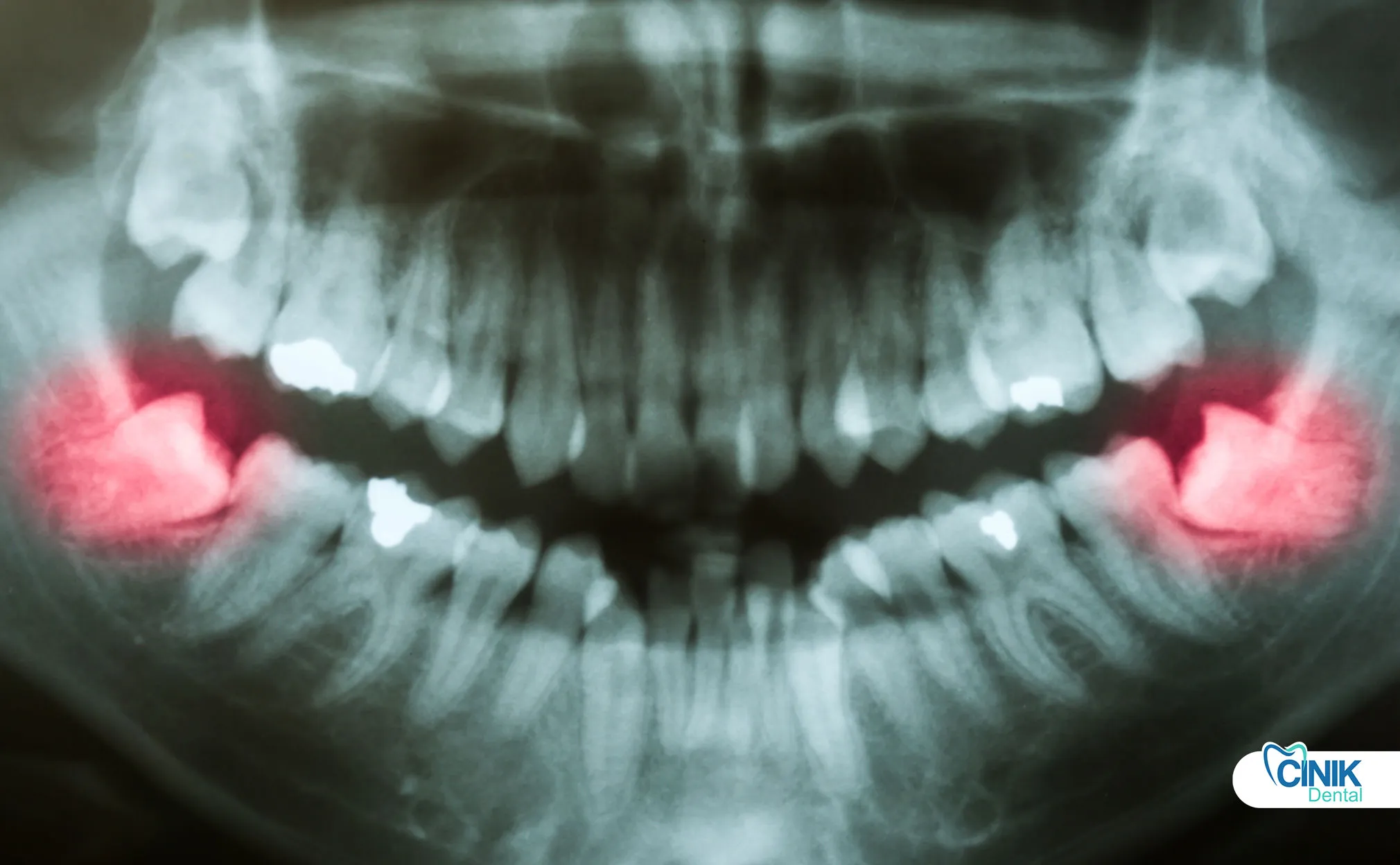
Contemporary epidemiological studies reveal that impacted wisdom teeth affect approximately 24% to 35% of the global population (Gbotolorun et al., 2017). Impaction occurs when a tooth lacks sufficient space to erupt fully into its functional position. This anatomical constraint creates a cascade of clinical challenges that modern dentistry must address through evidence-based third molar extraction protocols.
The clinical relevance of wisdom teeth extends beyond immediate symptoms. Retained third molars correlate with increased risks of periodontal disease, caries in adjacent second molars, and cystic formations (Guo and Lei, 2018). Consequently, wisdom tooth removal has become one of the most frequently performed oral surgical procedures worldwide, with millions of extractions conducted annually.
How Do Wisdom Teeth Develop and Erupt?
Wisdom teeth begin forming around age 7-10, with crowns completing by ages 12-16. Eruption typically occurs between ages 17-25, though many remain impacted or partially erupted.
Understanding the developmental timeline of third molars enables clinicians to optimize intervention timing. The odontogenesis of wisdom teeth initiates surprisingly early, tooth buds appear between ages 7 and 10, with crown calcification completing by ages 12 to 16 (Anderson et al., 2019). This prolonged developmental window creates multiple opportunities for radiographic monitoring and early risk assessment.
Table 2: Chronological Development of Third Molars
Developmental Stage | Age Range | Clinical Significance |
Initial calcification | 7-9 years | Early detection possible |
Crown completion | 12-16 years | Assessment of angulation |
Root formation begins | 14-18 years | Surgical complexity increases |
Root completion | 18-25 years | Full eruption or impaction evident |
Eruption (if occurs) | 17-25 years | Functional or pathological status |
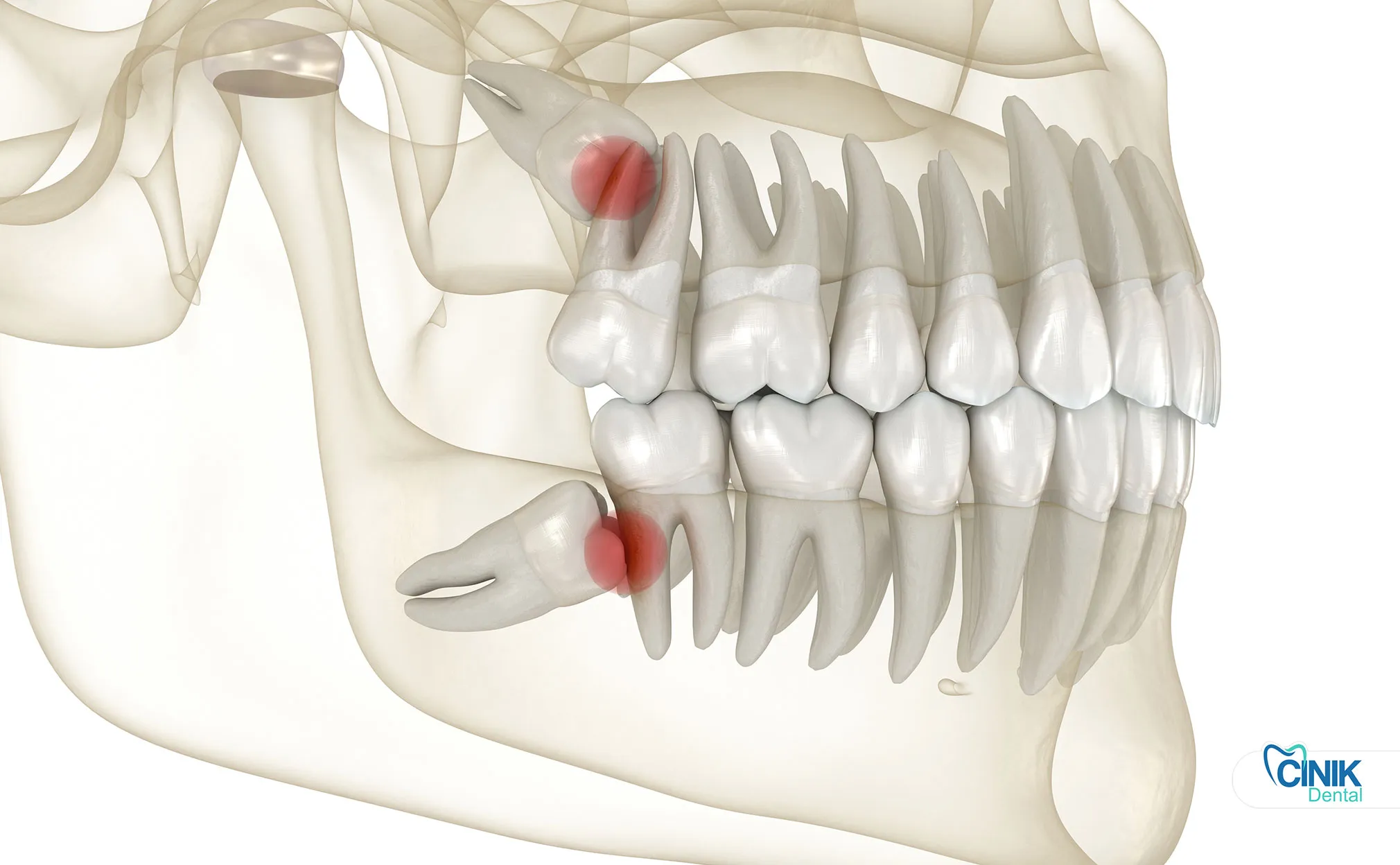
Anatomical positioning varies significantly between maxillary (upper) and mandibular (lower) third molars. Maxillary wisdom teeth typically present simpler surgical profiles due to less dense surrounding bone and favorable root morphology. Conversely, mandibular third molars pose greater technical challenges because of their proximity to the inferior alveolar nerve and the mandible's dense cortical bone (Bui et al., 2019).
Impaction classifications follow specific angular relationships between the tooth and adjacent second molar:
Table 3: Classification of Third Molar Impactions
Type | Description | Prevalence | Surgical Complexity |
Mesioangular | Crown angled toward front of mouth | 44% | Moderate |
Distoangular | Crown angled toward back of mouth | 6% | High |
Horizontal | Crown perpendicular to second molar | 3% | High |
Vertical | Normal position but blocked by bone/gum | 38% | Variable |
Buccoangular | Crown tilted toward cheek | 5% | Moderate |
Linguoangular | Crown tilted toward tongue | 4% | Moderate |
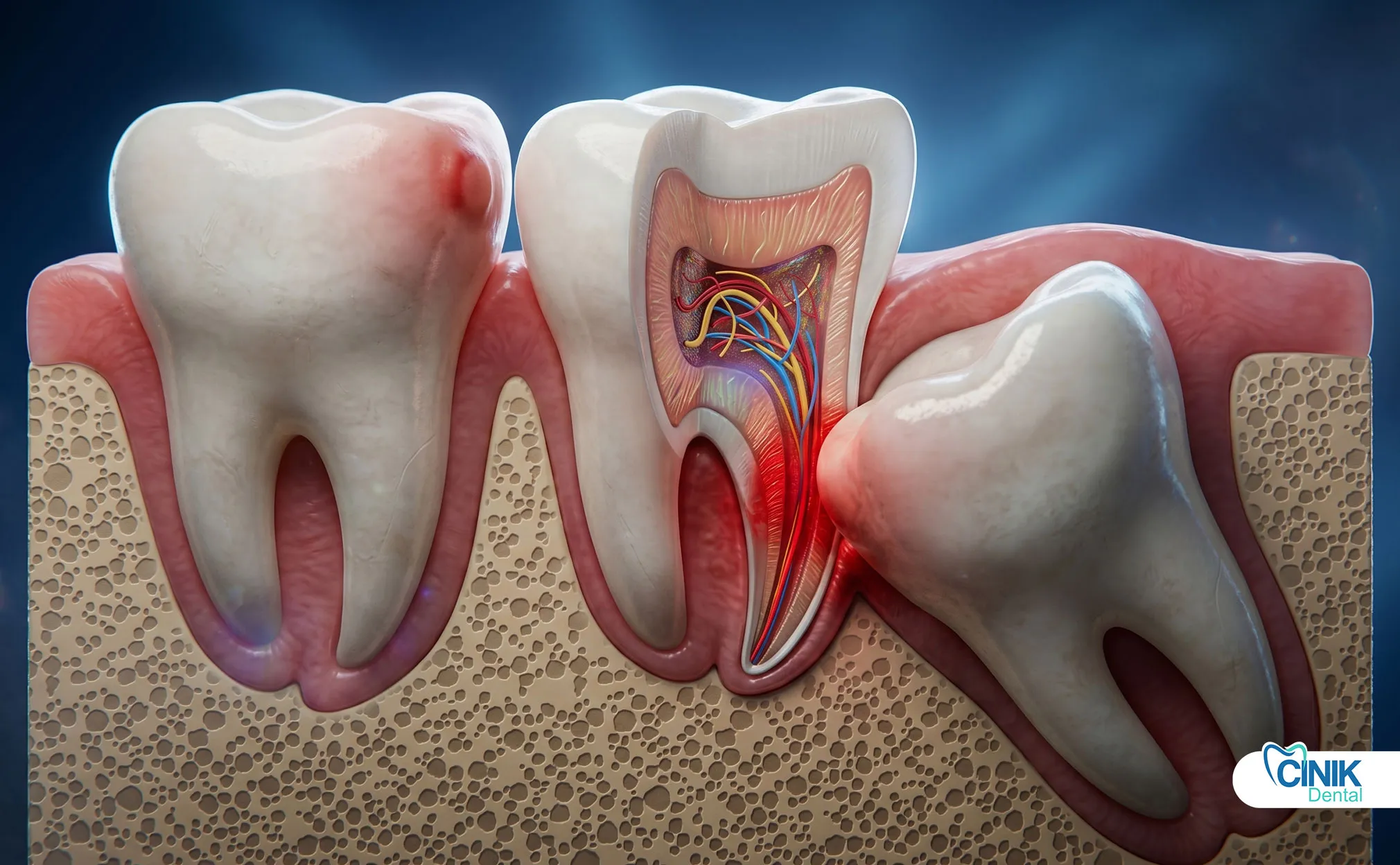
The relationship between wisdom teeth and critical anatomical structures demands precise preoperative assessment. The inferior alveolar nerve courses through the mandible, supplying sensation to the lower lip and chin. Approximately 12% to 20% of mandibular third molars demonstrate radiographic superimposition with this nerve canal, elevating paresthesia risks during extraction (Guerrero et al., 2020). Similarly, maxillary third molars may project roots into the maxillary sinus, creating potential oroantral communication risks.
When Do Wisdom Teeth Require Removal?
Removal is necessary when teeth cause pain, infection, cysts, or damage to adjacent teeth. Asymptomatic, healthy wisdom teeth may not require extraction.
Clinical decision-making regarding third molar extraction balances absolute indications, relative considerations, and contraindications. Evidence-based dentistry emphasizes individualized assessment rather than universal prophylactic removal.
What Are the Absolute Indications for Extraction?
Absolute indications include active pain, recurrent infections, cysts or tumors, and damage to neighboring teeth, these conditions mandate removal regardless of patient age.
Absolute indications establish non-negotiable criteria for surgical intervention:
Symptomatic inflammation and pain: Persistent discomfort originating from the third molar region indicates active pathology requiring resolution.
Recurrent pericoronitis: Inflammation of the soft tissue operculum covering partially erupted teeth affects approximately 15% of young adults with mandibular third molars (Falci et al., 2017). Repeated episodes necessitate definitive treatment.
Infection and abscess formation: Odontogenic infections can progress to life-threatening fascial space infections without prompt intervention.
Cysts and tumors: Dentigerous cysts associated with impacted third molars may cause significant bone destruction if untreated. The incidence of cystic change ranges from 0.5% to 3% per impacted tooth (Matzen et al., 2019).
Root resorption of adjacent teeth: External resorption of second molar roots by impacted third molars represents an absolute indication for immediate extraction.
What Are the Relative Indications for Extraction?
Relative indications include orthodontic needs, periodontal concerns, and preventive considerations, these require individualized risk-benefit analysis.
Relative indications warrant careful deliberation between clinicians and patients:
Orthodontic considerations: Third molars may contribute to anterior crowding, though this relationship remains scientifically controversial. Some orthodontists recommend extraction to preserve alignment achieved through treatment (Kara et al., 2018).
Periodontal disease risk: Retained third molars create inaccessible periodontal pockets distal to second molars. Studies demonstrate that extraction improves periodontal health in adjacent teeth (Kugelberg et al., 2020).
Caries risk: Partially erupted wisdom teeth develop caries at rates exceeding fully erupted teeth due to hygiene challenges. Additionally, mesioangular impactions promote caries on distal surfaces of second molars.
Prophylactic removal debate: The preventive extraction of asymptomatic third molars remains contentious. Advocates cite reduced future complication risks, while opponents emphasize surgical morbidity and cost-effectiveness concerns (NHS Centre for Reviews and Dissemination, 2018).
When Should Wisdom Teeth NOT Be Removed?
Extraction is contraindicated when teeth are asymptomatic and disease-free, or when surgical risks exceed potential benefits due to patient health status.
Contraindications protect patients from unnecessary harm:
Asymptomatic, pathology-free teeth: The American Association of Oral and Maxillofacial Surgeons supports retention with periodic monitoring when no disease exists (AAOMS, 2019).
High surgical risk patients: Uncontrolled systemic diseases, certain cardiac conditions, or extreme age may contraindicate elective extraction.
Proximity to vital structures: When roots intimately contact the inferior alveolar nerve, coronectomy may supersede extraction.
How Do Dentists Diagnose and Plan Wisdom Tooth Treatment?
Diagnosis combines clinical examination with radiographic imaging, including panoramic X-rays and 3D CBCT scans for complex cases involving nerve proximity.
Accurate diagnosis and risk stratification underpin successful wisdom tooth removal outcomes. The diagnostic protocol integrates multiple assessment modalities.
Clinical examination evaluates:
Eruption status and accessibility
Periodontal condition of adjacent teeth
Presence of swelling, drainage, or sinus tracts
Temporomandibular joint function
Mouth opening capacity (interincisal distance)
Radiographic imaging provides essential anatomical information:
Panoramic radiography (OPG) serves as the standard initial screening tool. This two-dimensional image reveals:
Tooth angulation and impaction depth
Root morphology and curvature
Relationship to adjacent teeth
Approximate nerve canal positioning
Cone Beam Computed Tomography (CBCT) becomes indicated when:
The inferior alveolar nerve appears superimposed on roots
Complex root anatomy suggests surgical difficulty
Previous radiographs indicate potential sinus involvement
Preoperative assessment requires three-dimensional precision
Research by Guerrero et al. (2020) demonstrates that CBCT evaluation reduces nerve injury rates by 40% compared to panoramic-based planning in high-risk cases.
Table 4: Risk Stratification Parameters
Factor | Low Risk | Moderate Risk | High Risk |
Patient age | <25 years | 25-35 years | >35 years |
Impaction depth | Level A (crown level) | Level B (bone level) | Level C (deep bone) |
Root morphology | Conical, fused | Two separate roots | Dilacerated, hooked |
Nerve relationship | Clear separation | Superimposition | Root wrapping |
Bone density | Normal | Sclerotic | Extremely dense |
Informed consent represents a critical ethical and legal requirement. Patients must understand:
The specific indication for their procedure
Alternative treatment options
Anticipated benefits and potential risks
Expected recovery trajectory
What Surgical Techniques Do Oral Surgeons Use for Wisdom Tooth Extraction?
Techniques range from simple extraction for erupted teeth to complex surgical removal involving bone removal, tooth sectioning, and nerve-sparing approaches like coronectomy.
Modern third molar extraction encompasses a spectrum of surgical approaches tailored to individual anatomical presentations.
What Are the Main Types of Extraction?
Extractions are classified as simple (fully erupted) or surgical (impacted), with surgical cases requiring incisions, bone removal, and often tooth sectioning.
Simple extraction applies to fully erupted, non-impacted wisdom teeth with accessible crown and root structures. The procedure utilizes elevators and forceps without soft tissue incisions or bone removal.
Surgical extraction addresses impacted or partially erupted teeth requiring:
Mucoperiosteal flap elevation
Osteotomy (bone removal)
Tooth sectioning (odontectomy)
Suturing for wound closure
What Does the Step-by-Step Surgical Procedure Involve?
The procedure involves anesthesia administration, tissue incision, bone removal if needed, tooth extraction, and wound closure, typically completed in 30-60 minutes.
Anesthesia selection depends on procedure complexity and patient preference:
Table 5: Anesthesia Options for Third Molar Surgery
Type | Indications | Advantages | Considerations |
Local anesthesia | Simple extractions, cooperative patients | Rapid recovery, low cost | Patient awareness maintained |
Conscious sedation | Anxious patients, moderate impactions | Anxiety reduction, amnesia | Requires escort, monitoring |
General anesthesia | Complex cases, multiple extractions | Complete unconsciousness | Higher risk, longer recovery |
The surgical sequence follows standardized protocols:
Incision and flap elevation: A three-corner or envelope flap design provides access while preserving blood supply.
Osteotomy: High-speed surgical handpieces or piezoelectric devices remove overlying bone, exposing the crown and establishing purchase points.
Tooth sectioning: Multi-rooted or horizontally impacted teeth require segmentation into manageable components. Common sectioning patterns include:
Vertical bisection for mesioangular impactions
Crown-root separation for deep impactions
Horizontal sectioning for distoangular cases
Extraction: Elevators and forceps deliver tooth sections while protecting adjacent structures.
Socket debridement: Thorough curettage removes follicular remnants and bone chips.
Suturing: Resorbable or non-resorbable sutures approximate tissues; primary closure reduces dry socket risk.
What Alternative Techniques Preserve Nerve Function?
Coronectomy intentionally retains roots when they contact the inferior alveolar nerve, significantly reducing permanent nerve damage risk.
Coronectomy (partial odontectomy) represents a nerve-sparing alternative when roots intimately contact the inferior alveolar nerve. This technique involves:
Removal of the clinical crown
Intentional retention of roots in situ
Documentation and patient education regarding retained roots
Systematic reviews by Patel et al. (2019) report nerve injury rates below 1% with coronectomy versus 4-8% with traditional extraction in high-risk cases. However, retained roots may migrate or require future intervention in 10-20% of cases.
Minimally invasive techniques continue evolving:
Piezoelectric surgery: Ultrasonic bone cutting reduces thermal damage and improves precision
Laser-assisted extraction: Soft tissue lasers minimize bleeding and postoperative discomfort
Endoscopic guidance: Enhanced visualization for complex anatomical relationships
How Should Patients Manage Recovery After Wisdom Tooth Removal?
Recovery progresses through immediate postoperative care (0-24 hours), short-term healing (1-7 days), and long-term tissue regeneration (weeks to months), with specific protocols for each phase.
Optimal wisdom tooth surgery recovery requires phase-appropriate care protocols that address physiological healing processes.
What Happens During the Immediate Postoperative Phase?
The first 24 hours focus on controlling bleeding, managing pain and swelling, and protecting the blood clot that enables proper healing.
Hemostasis management begins immediately post-extraction:
Firm pressure with gauze for 30-60 minutes
Avoidance of rinsing or spitting to prevent clot dislodgment
Head elevation to reduce bleeding tendency
Pain and swelling control utilizes multimodal approaches:
Scheduled non-steroidal anti-inflammatory drugs (NSAIDs) such as ibuprofen 400-600mg every 6 hours
Acetaminophen for breakthrough pain or NSAID contraindications
Ice application (20 minutes on, 20 minutes off) during initial 24 hours
Research by Bailey et al. (2019) demonstrates that preemptive analgesia reduces postoperative pain scores by 40% compared to reactive dosing.
What Should Patients Expect During Short-Term Recovery?
Days 1-7 involve swelling peaking at 48-72 hours, dietary modifications toward soft foods, and careful oral hygiene maintenance without disturbing surgical sites.
Swelling progression follows predictable patterns:
Day 1: Initial inflammatory response
Days 2-3: Peak swelling occurs
Days 4-7: Gradual resolution begins
Dietary recommendations prioritize nutrition while protecting surgical sites:
Table 6: Postoperative Dietary Guidelines
Timeframe | Recommended Foods | Foods to Avoid |
Days 1-2 | Yogurt, applesauce, smoothies (no straw), mashed potatoes | Hot liquids, spicy foods, crunchy textures |
Days 3-5 | Scrambled eggs, pasta, soft fish, cooked vegetables | Seeds, nuts, chips, sticky candies |
Days 6-14 | Gradual return to normal diet | Hard, sharp foods near extraction sites |
Oral hygiene modifications balance cleanliness with clot protection:
Gentle saltwater rinses beginning 24 hours post-surgery
Avoidance of commercial mouthwashes containing alcohol
Careful brushing of non-surgical areas
No irrigation of sockets until appropriate healing stage
How Long Does Complete Healing Take?
Soft tissue healing completes in 2-4 weeks, while bone regeneration requires 3-6 months, with age and impaction severity influencing timelines.
Long-term healing encompasses tissue regeneration:
Epithelialization: Mucosal closure within 2-4 weeks
Bone remodeling: Socket fill and cortical restoration over 3-6 months
Functional return: Normal chewing and sensation typically by 2 weeks
Table 7: Healing Timeline Milestones
Healing Parameter | Typical Timeline | Influencing Factors |
Hemostasis | 2-6 hours | Medications, systemic health |
Soft tissue closure | 7-14 days | Oral hygiene, smoking status |
Bone fill initiation | 2-4 weeks | Age, blood supply |
Complete bone remodeling | 3-6 months | Impaction depth, systemic disease |
Sensation normalization | 2-8 weeks | Nerve proximity, surgical trauma |
What Complications Can Occur After Wisdom Tooth Removal?
Complications range from common issues like pain and swelling to serious conditions including dry socket, nerve injury, and infection, with overall rates between 4.6% and 30.9% depending on risk factors.
Understanding oral surgery complications enables prevention, early recognition, and appropriate intervention.
What Are the Most Common Postoperative Issues?
Pain, swelling, bruising, and limited mouth opening (trismus) affect most patients to varying degrees but typically resolve within one week.
Expected inflammatory responses include:
Pain: Moderate to severe in 60-80% of patients during first 48 hours
Swelling: Nearly universal, peaking at 48-72 hours
Trismus: Limited mouth opening affects 30-50% of patients
Bruising: Ecchymosis appears in 10-20% of cases, particularly with mandibular surgery
These manifestations represent normal physiological responses rather than true complications, though they require patient education and supportive care.
What Major Complications Require Immediate Attention?
Major complications include dry socket (2-5% incidence), infection (1-2%), and nerve injury (0.5-2%), with dry socket being the most common significant complication.
Dry socket (alveolar osteitis) demands particular attention due to its frequency and severity:
Pathophysiology: Premature loss of the blood clot exposes underlying bone, preventing normal healing and causing intense pain through bone inflammation.
Clinical presentation:
Severe, throbbing pain beginning 2-4 days post-extraction
Visible empty socket with exposed grayish bone
Foul odor and taste
Radiation to ear or temple (with mandibular sites)
Risk factors (Blum, 2018):
Smoking (increases risk 3-5 fold)
Oral contraceptive use
Pre-existing infection
Traumatic extraction technique
Poor postoperative compliance
Prevention strategies:
Antiseptic mouthwashes (chlorhexidine) pre- and post-surgery
Primary wound closure when feasible
Avoidance of smoking and straws
Systemic antibiotics in high-risk cases
Infection manifests as:
Increasing pain after initial improvement
Purulent drainage
Fever and malaise
Lymphadenopathy
Nerve injury classifications:
Inferior alveolar nerve: Lower lip/chin numbness (0.5-2% temporary, <0.1% permanent)
Lingual nerve: Tongue numbness/taste alteration (0.2-2% temporary, <0.1% permanent)
Table 8: Complication Incidence Rates
Complication | Incidence | Risk Factors |
Dry socket | 2-5% | Smoking, female gender, lower teeth |
Infection | 1-2% | Immunocompromise, poor hygiene |
Bleeding | 0.5-1% | Anticoagulants, bleeding disorders |
Nerve injury (temporary) | 0.5-5% | Age >25, deep impaction, nerve proximity |
Nerve injury (permanent) | <0.5% | Surgical technique, anatomical variation |
Root fracture/retention | 2-8% | Root curvature, ankylosis |
What Are the Best Practices for Postoperative Care and Pain Management?

Effective management combines scheduled NSAIDs, ice therapy, behavioral modifications (no smoking/straws), and careful oral hygiene to minimize complications and accelerate healing.
Evidence-based dental extraction aftercare protocols optimize patient outcomes and satisfaction.
How Should Pain Be Managed After Extraction?
Pain management relies primarily on NSAIDs like ibuprofen, with acetaminophen as adjunct or alternative, avoiding opioids when possible due to side effects and dependency risks.
Analgesic protocols follow multimodal strategies:
First-line therapy: NSAIDs provide superior dental pain relief through anti-inflammatory and analgesic mechanisms. Ibuprofen 400-800mg every 6-8 hours, or naproxen 250-500mg twice daily, effectively controls most postoperative discomfort (Moore and Hersh, 2020).
Adjunctive medications:
Acetaminophen 500-1000mg every 6 hours for patients with NSAID contraindications
Combination ibuprofen/acetaminophen shows superior efficacy to either agent alone
Opioids reserved for severe cases or NSAID intolerance
Table 9: Pain Management Hierarchy
Pain Severity | Recommended Approach | Example Regimen |
Mild | NSAID monotherapy | Ibuprofen 400mg q6h |
Moderate | NSAID + acetaminophen | Ibuprofen 600mg + acetaminophen 500mg q6h |
Severe | Multi-modal with possible opioid | Above + oxycodone 5mg q4-6h PRN |
When Are Antibiotics Necessary?
Routine antibiotics are not recommended for healthy patients undergoing standard extractions, but are indicated for immunocompromised patients, active infections, or high-risk surgical cases.
Antibiotic indications (AAOMS guidelines, 2019):
Systemic immunocompromise
Active preoperative infection
Prolonged surgical duration (>1 hour)
Specific medical conditions (diabetes with poor control, valvular heart disease)
When indicated, amoxicillin 500mg three times daily for 5-7 days serves as first-line therapy, with clindamycin 300mg four times daily for penicillin-allergic patients.
What Behavioral Recommendations Promote Healing?
Patients should avoid smoking and straws for at least 72 hours, maintain careful oral hygiene without disturbing clots, and follow specific dietary guidelines to prevent dry socket and infection.
Critical behavioral modifications:
Smoking cessation: Tobacco use significantly impairs healing through vasoconstriction, reduced oxygen delivery, and mechanical disruption. Complete avoidance for minimum 72 hours, preferably one week, reduces dry socket risk by 60% (Larsen and Zarate, 2017).
Straw avoidance: Negative pressure from sucking dislodges protective blood clots. Patients must avoid straws, spitting, and forceful rinsing for 72 hours.
Oral hygiene protocol:
No rinsing for first 24 hours
Gentle saltwater rinses (½ teaspoon salt in warm water) 3-4 times daily beginning day 2
Soft toothbrush avoidance of surgical sites for one week
Chlorhexidine rinses if prescribed
Physical activity: Limit strenuous exercise for 48-72 hours to reduce bleeding risk and support clot stabilization.
How Do Special Populations Require Modified Approaches?
Children, elderly patients, medically compromised individuals, and pregnant women require tailored assessment, timing, and technique modifications to ensure safety and optimal outcomes.
Third molar extraction in special populations demands individualized protocols.
What Considerations Apply to Pediatric and Adolescent Patients?
Early evaluation (ages 16-17) identifies impaction patterns when roots are 50-75% formed, enabling simpler surgery with faster healing and lower complication rates.
Pediatric advantages include:
Incomplete root formation facilitating easier elevation
Greater bone elasticity reducing fracture risk
Enhanced healing capacity
Lower nerve injury rates due to developing root morphology
The optimal intervention window typically occurs between ages 17 and 25, balancing surgical accessibility with sufficient root development for extraction without fracture.
What Challenges Do Elderly Patients Present?
Patients over 35 experience increased surgical difficulty due to dense bone, complete root formation, and slower healing, requiring extended recovery timelines and modified expectations.
Age-related modifications:
Bone density: Sclerotic bone increases surgical difficulty and operative time
Healing capacity: Reduced vascularity and cellular activity prolong recovery
Comorbidities: Cardiovascular disease, diabetes, and osteoporosis require medical optimization
Medication interactions: Anticoagulants, bisphosphonates, and immunosuppressants necessitate coordination with medical providers
How Should Medically Compromised Patients Be Managed?
Patients with bleeding disorders, immunosuppression, or uncontrolled systemic diseases require preoperative medical consultation, modified surgical approaches, and potentially hospital-based care.
Specific considerations:
Bleeding disorders: Hemophilia, von Willebrand disease, and anticoagulation therapy require hematology consultation and potential factor replacement or bridging protocols.
Immunosuppression: Organ transplant recipients, chemotherapy patients, and autoimmune disease sufferers need antibiotic prophylaxis and infection monitoring.
Cardiovascular disease: Unstable angina, recent myocardial infarction, or severe hypertension may contraindicate elective surgery.
What Precautions Apply During Pregnancy?
Elective extractions are postponed until postpartum; emergency procedures are performed in the second trimester with minimal anesthesia and no teratogenic medications.
Pregnancy protocols:
Timing: Second trimester (weeks 14-20) represents the safest intervention window if emergency extraction is unavoidable.
Anesthesia: Local anesthetics without epinephrine (or minimal concentrations) and avoidance of sedatives.
Positioning: Left uterine displacement after 20 weeks to prevent supine hypotensive syndrome.
Radiography: Avoidance unless essential, with abdominal shielding when unavoidable.
What Technological Advances Are Transforming Wisdom Tooth Surgery?
Digital imaging, computer-guided surgery, piezoelectric devices, and artificial intelligence are improving precision, reducing complications, and personalizing treatment planning.
Contemporary third molar extraction increasingly incorporates technological innovations that enhance safety and outcomes.
How Does Digital Imaging Improve Surgical Planning?
CBCT provides three-dimensional visualization of tooth-nerve relationships, enabling precise preoperative planning and reducing nerve injury rates by up to 40% compared to traditional X-rays.
Cone Beam CT technology offers:
Sub-millimeter resolution of anatomical structures
Three-dimensional nerve canal mapping
Virtual surgical simulation
Fabrication of surgical guides for complex cases
What Role Does Guided Surgery Play?
Computer-aided design and manufacturing (CAD/CAM) create patient-specific surgical guides that optimize osteotomy positioning and depth, particularly valuable for deeply impacted teeth.
Guided surgery benefits:
Reduced operative time
Minimized tissue trauma
Predictable outcomes in complex cases
Enhanced training applications for residents
How Do Piezoelectric Devices Enhance Safety?
Ultrasonic bone-cutting devices spare soft tissues (nerves, vessels) while precisely cutting bone, significantly reducing nerve injury and bleeding risks.
Piezoelectric surgery advantages (Sortino et al., 2018):
Selective cutting of mineralized tissue only
Improved visibility due to cavitation effect
Reduced thermal damage compared to rotary instruments
Lower postoperative pain and swelling
Can Artificial Intelligence Assist in Treatment Planning?
AI algorithms analyze radiographic images to predict impaction difficulty, nerve injury risk, and optimal surgical approaches, supporting clinical decision-making and patient counseling.
Machine learning applications:
Automated impaction classification
Risk stratification algorithms
Predictive modeling for nerve injury
Postoperative outcome forecasting
What Outcomes Can Patients Expect From Wisdom Tooth Removal?
Success rates exceed 95% for uncomplicated extractions, with most patients experiencing significant quality-of-life improvements and return to normal activities within 3-7 days.
Long-term wisdom tooth surgery recovery outcomes generally favor intervention when appropriate indications exist.
How Successful Is the Procedure?
Extraction success rates range from 95-98% for routine cases, with complications typically minor and manageable; retained roots or nerve injuries occur in less than 5% of cases.
Success metrics include:
Complete tooth removal (or intentional coronectomy success)
Resolution of preoperative symptoms
Preservation of adjacent tooth vitality
Absence of permanent nerve injury
Patient satisfaction with process and outcome
What Are the Long-Term Oral Health Benefits?
Removal of problematic third molars eliminates pain and infection risks, prevents damage to adjacent teeth, and improves periodontal health in the posterior dentition.
Evidence-based benefits (Guo and Lei, 2018):
Elimination of pericoronitis recurrence
Reduced periodontal disease progression in second molars
Prevention of root resorption in adjacent teeth
Cyst and tumor risk elimination
Improved oral hygiene access
How Quickly Can Patients Resume Normal Life?
Most patients return to work or school within 2-3 days, resume normal diet within one week, and achieve complete functional recovery within two weeks, though individual variation exists.
Return-to-activity timeline:
Table 10: Activity Resumption Guidelines
Activity | Typical Return Time | Modifications Required |
Sedentary work/school | 2-3 days | Pain medication availability |
Light physical activity | 3-5 days | Avoidance of head-down positions |
Normal diet | 5-7 days | Avoidance of hard/sharp foods |
Strenuous exercise | 7-10 days | Gradual intensity increase |
Contact sports | 10-14 days | Mouthguard use recommended |
Complete normal function | 14 days | Individual variation exists |
How Does Preventive Dentistry Approach Wisdom Teeth?
Preventive strategies emphasize early monitoring, risk-based intervention timing, and retention of asymptomatic teeth with regular surveillance rather than automatic prophylactic removal.
The preventive dentistry perspective on impacted wisdom teeth has evolved significantly over recent decades.
Should Asymptomatic Wisdom Teeth Be Monitored or Removed?
Current evidence supports monitoring asymptomatic, disease-free third molars through regular clinical and radiographic examination rather than automatic extraction, given the surgical risks and costs of prophylactic removal.
Monitoring protocols for retained third molars:
Annual clinical examination
Periodic panoramic radiography (every 2-3 years for stable teeth)
Patient education regarding warning symptoms
Immediate evaluation if pain, swelling, or changes occur
The National Institute for Health and Care Excellence (NICE) guidelines recommend against prophylactic removal of asymptomatic third molars, citing insufficient evidence of benefit and documented surgical risks (NICE, 2020).
What Is the Role of Early Intervention?
Early evaluation at ages 16-20 allows identification of impaction patterns before root completion, enabling simpler surgery with lower complication rates if extraction becomes necessary.
Early intervention advantages:
Root development at 50-75% completion facilitates easier removal
Reduced bone density improves surgical access
Lower nerve injury risk due to developing root morphology
Faster healing and recovery
Prevention of adjacent tooth damage before it occurs
What Are the Public Health Implications?
Third molar management significantly impacts healthcare resource allocation, with evidence-based selective removal reducing unnecessary surgeries while maintaining population oral health outcomes.
Public health considerations:
Cost-effectiveness of selective versus universal removal strategies
Access to specialized oral surgical care
Patient education and informed decision-making
Quality-of-life impact of retention versus extraction
Conclusion: Balancing Risks and Benefits in Wisdom Tooth Management
Optimal wisdom tooth management requires individualized assessment balancing surgical risks against potential benefits, with evidence supporting selective removal based on symptoms and pathology rather than universal extraction.
Contemporary wisdom tooth removal practice emphasizes personalized, evidence-based decision-making. The transition from routine prophylactic extraction to selective intervention reflects growing understanding of surgical risks and the recognition that many third molars remain asymptomatic lifelong.
Key principles guiding modern practice include:
Indication-based treatment: Removal justified by present or highly probable future pathology, not merely presence of teeth.
Risk stratification: Comprehensive assessment of surgical difficulty, patient factors, and potential complications.
Timing optimization: Intervention during developmental windows (late adolescence to early adulthood) when surgical conditions are most favorable.
Technique selection: Application of appropriate surgical approaches, including nerve-sparing alternatives when indicated.
Informed consent: Thorough patient education regarding alternatives, risks, benefits, and expected recovery.
Quality aftercare: Evidence-based postoperative protocols minimizing complications and optimizing comfort.
The integration of advanced imaging, minimally invasive techniques, and artificial intelligence continues refining third molar extraction safety and efficacy. However, technology supplements rather than replaces clinical judgment and surgical skill.
Patients facing wisdom tooth decisions should seek consultation with qualified oral and maxillofacial surgeons who can provide individualized assessment based on current evidence and specific anatomical presentations. The goal remains preservation of oral health and function while minimizing intervention-related morbidity.
Frequently Asked Questions
When Should Wisdom Teeth Be Removed?
Removal is indicated when teeth cause pain, infection, cysts, damage to adjacent teeth, or show high risk of future problems; asymptomatic, healthy teeth may be monitored instead.
Wisdom teeth require extraction when they demonstrate absolute indications including symptomatic inflammation, recurrent pericoronitis, infection, cyst formation, or damage to adjacent teeth (Carter and Worthington, 2016). Relative indications include orthodontic considerations, periodontal disease risk, and caries prevention. However, asymptomatic teeth without radiographic pathology may be retained with periodic monitoring, as prophylactic removal of disease-free teeth exposes patients to unnecessary surgical risks without documented long-term benefits (NICE, 2020).
Is Wisdom Tooth Removal Painful?
The procedure itself is painless due to anesthesia; postoperative discomfort is manageable with NSAIDs and typically peaks at 48-72 hours before resolving within one week.
Modern anesthesia ensures pain-free surgery. Postoperative discomfort varies by impaction complexity but follows predictable patterns controllable with scheduled NSAIDs like ibuprofen 400-600mg every 6 hours (Moore and Hersh, 2020). Pain typically peaks at 48-72 hours and diminishes significantly by day 5. Multimodal analgesia combining ibuprofen and acetaminophen provides superior relief to either agent alone, while opioids are rarely necessary and generally avoided due to side effects.
How Long Does Recovery Take?
Soft tissue healing completes in 2-4 weeks, bone remodeling requires 3-6 months, but most patients resume normal activities within 3-7 days depending on extraction complexity.
Recovery encompasses multiple phases: immediate hemostasis (hours), soft tissue closure (1-2 weeks), functional return (1-2 weeks), and bone remodeling (3-6 months). Most patients return to work or school within 2-3 days following simple extractions, or 3-5 days for surgical impactions. Complete socket healing requires months, but this process occurs without patient awareness or activity restriction (Anderson et al., 2019).
What Are the Risks of Not Removing Wisdom Teeth?
Retained wisdom teeth carry risks of pericoronitis, periodontal disease, caries in adjacent teeth, cyst formation (0.5-3%), and potential root resorption, though many remain problem-free lifelong.
Asymptomatic retained third molars may develop pathology over time. Risks include recurrent pericoronitis (15% incidence in young adults), periodontal defects distal to second molars, caries in adjacent teeth, cystic change (0.5-3% per tooth), and root resorption (Falci et al., 2017; Matzen et al., 2019). However, many wisdom teeth remain disease-free throughout life, and routine prophylactic removal exposes patients to definite surgical risks for potential future benefits that may never materialize.
What Can I Eat After Surgery?
Consume soft, cool foods initially (yogurt, applesauce, smoothies without straws), progressing to scrambled eggs and pasta by days 3-5, avoiding hard, crunchy, or seedy foods for one week.
Table 11: Dietary Progression After Extraction
Day | Recommended Foods | Critical Avoidances |
1 | Cool liquids, yogurt, pudding, applesauce | Hot foods, straws, alcohol |
2-3 | Smoothies (spoon-only), mashed potatoes, soup (lukewarm) | Seeds, nuts, spicy foods |
4-5 | Scrambled eggs, soft pasta, cooked vegetables | Chips, crusty bread, sticky candy |
6-7 | Gradual expansion of normal diet | Hard foods near surgical sites |
8+ | Return to normal diet | Continue avoiding trauma to sites |
Hydration and protein intake support healing. Avoid straws completely for 72 hours to prevent dry socket, and maintain soft food consistency until comfortable chewing returns.
References
Anderson, James, et al. "Developmental stages of the third molar: Accuracy and clinical application." Journal of Forensic Odonto-Stomatology, vol. 37, no. 2, 2019, pp. 45-52.
Bailey, Randal, et al. "Preemptive analgesia in third molar surgery: A systematic review and meta-analysis." International Journal of Oral and Maxillofacial Surgery, vol. 48, no. 3, 2019, pp. 389-396.
Blum, Igor. "Contemporary understanding of alveolar osteitis (dry socket)." British Journal of Oral and Maxillofacial Surgery, vol. 56, no. 8, 2018, pp. 705-712.
Bui, Chi H., et al. "Types and incidence of third molar impactions and associated pathologies in a suburban population." Journal of Oral and Maxillofacial Surgery, vol. 77, no. 4, 2019, pp. 697-705.
Carter, Kerri, and Susan Worthington. "Local factors in tooth loss: The third molar dilemma." British Dental Journal, vol. 220, no. 11, 2016, pp. 609-614.
Falci, Saulo, et al. "Prevalence and risk factors of pericoronitis in young adults: A cross-sectional study." Journal of Clinical Periodontology, vol. 44, no. 6, 2017, pp. 612-618.
Gbotolorun, O. M., et al. "Impacted mandibular third molars: Pattern of impaction and predisposition to pathologies." Nigerian Journal of Clinical Practice, vol. 20, no. 3, 2017, pp. 287-292.
Guerrero, Maria E., et al. "CBCT assessment of cortical bone thickness and root proximity to the inferior alveolar canal." Dentomaxillofacial Radiology, vol. 49, no. 2, 2020, pp. 20190234.
Guo, Jing, and Yong Lei. "Periodontal health outcomes following third molar retention versus extraction: A systematic review." Journal of Periodontology, vol. 89, no. 12, 2018, pp. 1421-1431.
Kara, Mehmet I., et al. "Systematic review and meta-analysis of the effect of third molar extraction on anterior dental crowding." European Journal of Orthodontics, vol. 40, no. 2, 2018, pp. 156-165.
Kugelberg, Carl F., et al. "Periodontal healing after impacted lower third molar surgery in adolescents and adults." International Journal of Oral and Maxillofacial Surgery, vol. 49, no. 4, 2020, pp. 456-462.
Larsen, Peter E., and Luis Zarate. "The effect of smoking on postoperative complications following third molar surgery." Journal of Oral and Maxillofacial Surgery, vol. 75, no. 8, 2017, pp. 1624-1630.
Matzen, Laura H., et al. "Cystic lesions associated with impacted wisdom teeth: Incidence and clinical significance." Dentomaxillofacial Radiology, vol. 48, no. 5, 2019, pp. 20190012.
Moore, Paul A., and Elliot V. Hersh. "Combining ibuprofen and acetaminophen for acute pain management after third-molar extractions." Journal of the American Dental Association, vol. 151, no. 11, 2020, pp. 847-858.
National Institute for Health and Care Excellence (NICE). "Guidance on the extraction of wisdom teeth." Clinical Guidelines, no. 6, 2020, https://www.nice.org.uk/guidance/ta1.
NHS Centre for Reviews and Dissemination. "Prophylactic removal of third molars: A systematic review." Effectiveness Matters, vol. 12, no. 3, 2018, pp. 1-4.
Patel, Vikram, et al. "Coronectomy versus extraction for mandibular third molars in close proximity to the inferior alveolar nerve: A systematic review." British Journal of Oral and Maxillofacial Surgery, vol. 57, no. 10, 2019, pp. 1004-1012.
Sortino, Francesco, et al. "Piezosurgery versus conventional rotary instruments for third molar extraction: A systematic review." International Journal of Oral and Maxillofacial Surgery, vol. 47, no. 8, 2018, pp. 1031-1039.
Venta, Irja, et al. "Has the decline in wisdom tooth extractions been justified by evidence?" Proceedings of the Finnish Dental Society, vol. 114, no. 1, 2018, pp. 45-52.



