
Tooth nerve death (pulp necrosis) occurs when the dental pulp, containing nerves and blood vessels, loses its vitality due to infection, trauma, or decay, leading to potential pain, discoloration, and infection if untreated.
What Happens When a Tooth Nerve Dies? (Pathophysiology)
The pulp loses blood supply and oxygen, leading to tissue breakdown, bacterial colonization, and eventual necrosis.
What Is Dental Pulp and Its Function?
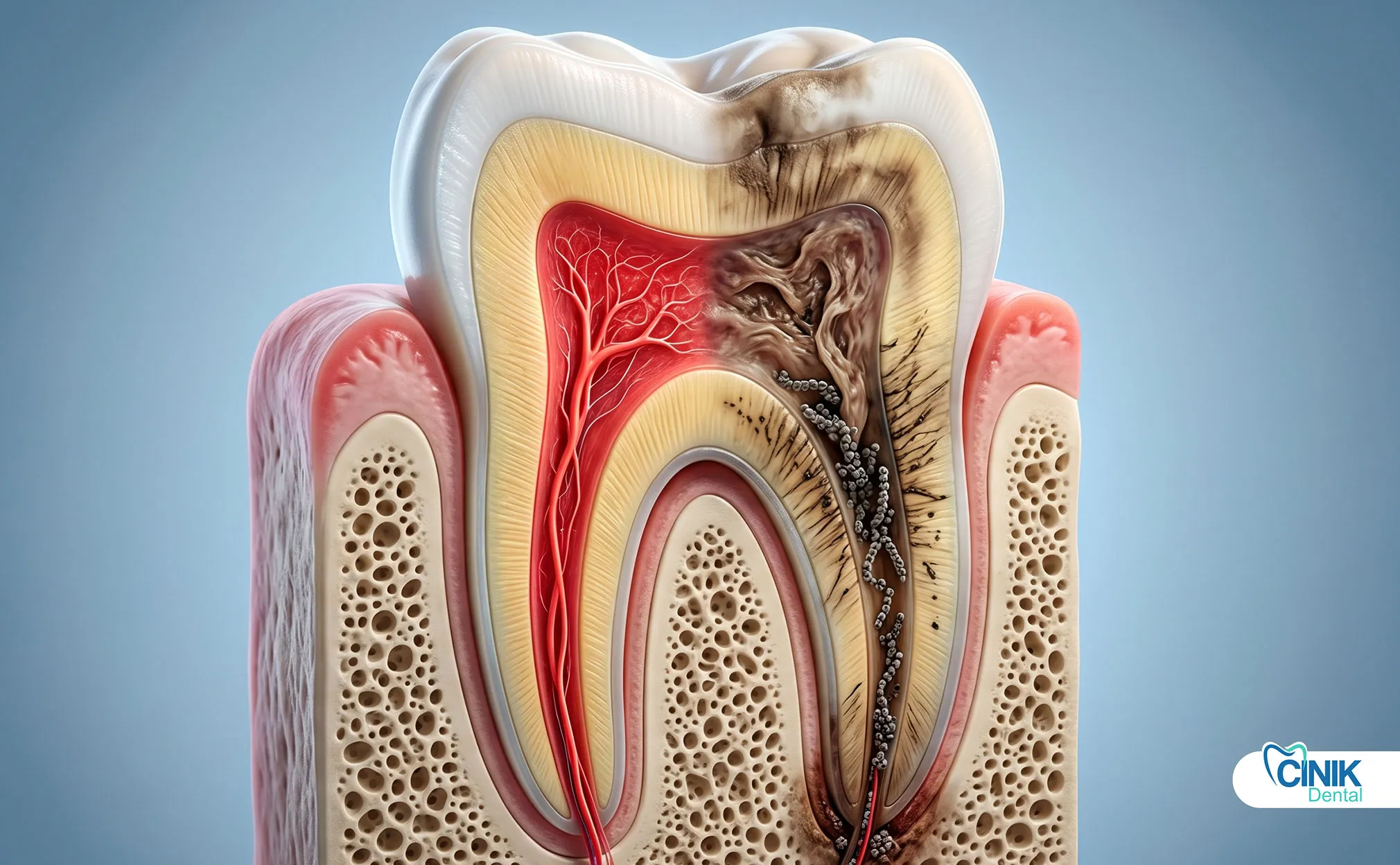
The dental pulp sits at the very center of your tooth. This soft tissue contains nerves, blood vessels, and connective tissue. It keeps your tooth alive and healthy.
The pulp performs three critical jobs. First, it maintains tooth vitality by delivering oxygen and nutrients through blood vessels. Second, it responds to temperature changes, pressure, and pain through an extensive nerve network. Third, it defends against bacterial invasion through immune cells that patrol the pulp chamber (Bergenholtz, 2019).
Think of the pulp as the heart of your tooth. Without it, the tooth becomes a hollow shell. The pulp chamber extends from the crown down through narrow canals in the tooth roots. This complex anatomy makes the pulp vulnerable to damage from multiple directions.
How Does Pulp Necrosis Develop?
Pulp necrosis follows a predictable pattern. The process starts with reversible pulpitis. At this stage, the pulp becomes inflamed but can still recover. You feel sharp pain when eating ice cream or drinking hot coffee. Remove the irritant, and the pulp heals.
If irritation continues, reversible pulpitis advances to irreversible pulpitis. The inflammation becomes permanent. Blood vessels swell and cut off their own blood supply. Pressure builds inside the rigid pulp chamber. This stage causes intense, lingering pain that keeps you awake at night.
Eventually, the blood supply stops completely. The pulp tissue dies. Bacteria move in and feed on the dead tissue. They release toxins that leak out through the root tip. This marks the beginning of pulp necrosis (Taha & Abdellatif, 2021).
Why Dead Teeth Can Still Cause Pain
Many patients feel confused. They ask: "If the nerve is dead, why does my tooth still hurt?"
The answer lies in the tissues surrounding the tooth. The dead pulp no longer registers pain. However, the infection spreads to the bone and ligaments around the root tip. These tissues contain plenty of living nerves. They scream in protest as pus builds up and pressure increases.
This explains why some necrotic teeth cause severe pain while others cause none at all. The pain depends on whether the infection has spread beyond the tooth itself.
What Causes Tooth Nerve Death?

The most common causes are deep decay, trauma, cracks, and repeated dental procedures allowing bacteria to reach the pulp.
Primary Causes
Deep Dental Caries: Cavities cause most cases of pulp necrosis. Bacteria eat through enamel and dentin. They reach the pulp and trigger inflammation. The deeper the cavity, the higher the risk. A small surface cavity takes months or years to reach the pulp. Once bacteria breach the pulp chamber, necrosis becomes likely (Ricucci et al., 2018).
Dental Trauma: A blow to the face can kill a tooth nerve instantly. Sports injuries, car accidents, and falls damage the blood vessels entering the tooth root. Even without visible cracks, the internal blood supply fails. Trauma can cause immediate necrosis or delayed death months later.
Cracked or Fractured Teeth: Cracks create highways for bacteria. They also irritate the pulp directly. Vertical root fractures often doom the tooth to necrosis. Patients who grind their teeth face higher risks of cracks that lead to pulp death.
Failed Restorations: Large fillings and repeated dental work stress the pulp. Each drilling episode causes inflammation. Over time, this cumulative trauma exhausts the pulp's ability to recover. Old fillings with gaps allow bacterial leakage underneath.
Secondary & Contributing Factors
Gum Disease: Periodontal disease creates deep pockets around tooth roots. Bacteria travel from these pockets into the pulp through lateral canals. This pathway causes necrosis even in teeth without cavities.
Enamel Wear: Aggressive brushing, acidic drinks, and teeth grinding strip away protective enamel. Thin enamel allows faster bacterial penetration. Bruxism also creates micro-cracks that harbor bacteria.
Poor Oral Hygiene: High bacterial loads in the mouth increase cavity risk. Plaque buildup produces acids that dissolve tooth structure. The more bacteria present, the faster decay progresses toward the pulp.
Systemic Factors: Smoking reduces blood flow to oral tissues. Diabetes impairs immune responses. Both conditions slow healing and increase necrosis risk. Some medications also affect oral health and pulp vitality.
Risk Factors
Risk Factor | Why It Matters | Prevention Strategy |
Untreated cavities | Bacteria reach pulp over time | Early filling placement |
Previous root canal | Tooth already compromised | Regular monitoring |
Large existing fillings | More tooth structure lost | Replacement before failure |
High sugar diet | Feels decay-causing bacteria | Dietary modification |
Trauma history | Blood supply already damaged | Mouthguard use |
What Are the Symptoms of a Dead Tooth Nerve?
Symptoms vary from severe pain to no pain at all, often including discoloration, swelling, or infection.
Early Symptoms (Dying Nerve)
Your body sends warning signals before the nerve dies completely. Pay attention to these early signs.
Temperature Sensitivity: You feel sharp pain when drinking hot coffee or eating ice cream. The pain lingers for several seconds after the temperature stimulus ends. This differs from normal sensitivity that stops immediately.
Spontaneous Pain: The tooth hurts without any trigger. You wake up at night with throbbing pain. This indicates irreversible pulpitis moving toward necrosis.
Biting Discomfort: Pressure on the tooth causes pain. The ligaments around the tooth root become inflamed. You start chewing on the other side of your mouth to avoid the sore tooth.
Advanced Symptoms (Necrotic Tooth)
Once the nerve dies, new symptoms appear.
Tooth Discoloration: The tooth turns grey, brown, or black. This happens because dead blood cells break down inside the tooth. The discoloration usually appears two to three weeks after nerve death. Front teeth show this most obviously (Plotino et al., 2017).
Persistent Pain: The pain changes character. Instead of sharp sensitivity, you feel dull, throbbing ache. The pain may come and go as infection pressure builds and releases.
Bad Taste or Odor: Pus draining from the tooth creates a foul taste. You may notice bad breath that does not improve with brushing. This indicates an active infection.
Gum Swelling: A pimple-like bump appears on the gums near the tooth root. This "gum boil" represents a drainage pathway for pus. Pressing it may release foul-tasting fluid.
Asymptomatic Cases
Not all dead teeth cause pain. Some patients feel nothing at all. The nerve dies quietly. The infection spreads slowly without triggering pain receptors. Dentists often discover these cases during routine X-rays. The image shows a dark area around the root tip indicating bone loss from chronic infection.
This silent progression makes regular dental check-ups essential. Waiting for pain means waiting too long.
How Is Tooth Nerve Death Diagnosed?
Diagnosis involves clinical examination, vitality tests, and radiographic imaging.
Clinical Examination
Your dentist starts with visual inspection. They look for color changes in the tooth. They check for swelling or drainage on the gums. They tap on the tooth with a dental instrument. A necrotic tooth often feels different, either more sensitive or completely numb to percussion.
The dentist also examines neighboring teeth. This helps determine exactly which tooth causes the problem. Pain can refer to other areas, making source identification tricky.
Diagnostic Tests
Thermal Testing: The dentist applies cold or heat to the tooth. A healthy tooth responds quickly. The sensation fades within seconds. A necrotic tooth shows no response. An inflamed tooth shows exaggerated, lingering pain.
Electric Pulp Testing: This device sends a mild electrical current through the tooth. Living nerves respond with a tingling sensation. Dead nerves feel nothing. This test works best on teeth without metal restorations.
Radiographs: X-rays reveal what eyes cannot see. They show dark areas around root tips indicating bone destruction from infection. They reveal deep decay approaching the pulp. They identify cracks that extend below the gum line. Digital radiographs reduce radiation exposure while providing detailed images (Cotti & Campisi, 2020).
Differential Diagnosis
Dentists must distinguish between several conditions with similar symptoms:
Condition | Nerve Status | Key Differentiator | Treatment |
Reversible pulpitis | Alive | Pain stops immediately when stimulus removed | Filling |
Irreversible pulpitis | Dying | Lingering pain, spontaneous episodes | Root canal |
Pulp necrosis | Dead | No response to vitality tests | Root canal or extraction |
Periodontal abscess | Variable | Deep gum pockets, different pain location | Periodontal treatment |
What Happens If a Dead Tooth Is Left Untreated?
Untreated necrosis leads to infection, abscess, bone loss, and possible systemic complications.
Local Complications
Dental Abscess: The infection forms a pocket of pus at the root tip. Pressure builds until the pus finds an escape route. It may drain through the gums or into surrounding tissues. Abscesses cause severe pain and facial swelling.
Bone Loss: Chronic infection destroys the bone holding the tooth. X-rays show expanding dark areas around the root. Advanced bone loss makes tooth saving impossible. The tooth loosens and may fall out.
Tooth Fracture: Dead teeth become brittle. Without the pulp's moisture, dentin dries out. The tooth cracks more easily under chewing forces. A vertical fracture often requires extraction.
Systemic Risks
Infection rarely stays localized. Bacteria enter the bloodstream. They travel to other body areas.
Spread to Jaw and Sinuses: Lower teeth infections move into the jawbone. Upper teeth infections reach the maxillary sinuses. Sinus infections cause facial pain and pressure. Jaw infections threaten airway patency in severe cases.
Sepsis Risk: While rare, dental infections can cause life-threatening sepsis. Your body's overwhelming response to infection damages multiple organs. People with weakened immune systems face higher risks (Lockhart et al., 2019).
Chronic Infection Impact
Long-standing infections create constant low-grade inflammation. This affects overall health. Research links chronic oral infections to heart disease and diabetes complications. The oral microbiome becomes unbalanced. Harmful bacteria dominate. This increases risks for new cavities and gum disease.
How Is Tooth Nerve Death Treated?

Treatment includes root canal therapy or extraction depending on the severity.
Root Canal Treatment (Gold Standard)
Root canal therapy saves most necrotic teeth. The procedure removes the dead pulp. It eliminates the infection source. It allows you to keep your natural tooth.
Step 1: Access and Removal: The dentist creates an opening through the tooth crown. They remove the necrotic pulp tissue using specialized instruments. They clean the entire canal system.
Step 2: Disinfection: Irrigating solutions flush bacteria from the canals. The dentist shapes the canals to receive filling material. This step determines treatment success. Thorough disinfection prevents reinfection.
Step 3: Sealing: The dentist fills the clean canals with gutta-percha, a rubber-like material. They seal the access cavity with a temporary or permanent filling.
Step 4: Restoration: Most root-canaled teeth need crowns. The crown protects the weakened tooth from fracture. It restores normal chewing function. Without a crown, the tooth may crack and require extraction (Siqueira & Rôças, 2020).
Tooth Extraction
Some teeth cannot be saved. Extraction becomes necessary when:
The tooth has a vertical root fracture
Bone loss exceeds 50% of root support
The tooth cannot be properly restored
Root canal treatment fails repeatedly
After extraction, you need tooth replacement. Options include dental implants, bridges, or partial dentures. Implants provide the most natural function and appearance. They also preserve jawbone density.
Adjunctive Treatments
Antibiotics: Dentists prescribe antibiotics when infection spreads beyond the tooth. They reduce swelling and control systemic symptoms. However, antibiotics alone do not cure pulp necrosis. The dead pulp remains a bacterial reservoir. Definitive treatment requires root canal or extraction.
Pain Management: Over-the-counter medications control post-treatment discomfort. Ibuprofen reduces both pain and inflammation. Acetaminophen provides additional relief. Most patients resume normal activities within 24 hours.
Can a Dead Tooth Be Saved?
Yes, most necrotic teeth can be preserved with timely root canal treatment.
Prognosis Factors
Several factors determine whether a necrotic tooth survives long-term:
Extent of Infection: Limited infection confined to the pulp chamber offers the best prognosis. Infection spreading into surrounding bone complicates treatment. Large abscesses require longer healing periods.
Bone Involvement: Teeth with minimal bone loss respond well to treatment. Advanced bone destruction compromises tooth stability. The tooth may need extraction despite successful root canal therapy.
Timing of Treatment: Early intervention prevents complications. Delay allows infection to spread. It reduces bone support. It increases fracture risk. Prompt treatment saves more teeth.
Tooth Location: Front teeth have single, straight canals. They treat more predictably than molars with multiple, curved canals. However, modern techniques handle complex anatomy successfully.
Success Rates
Research demonstrates high success rates for root canal treatment on necrotic teeth:
Time Frame | Success Rate | Study |
2 years | 94% | Ng et al. (2011) |
4 years | 91% | Ng et al. (2011) |
6-8 years | 86% | Ng et al. (2011) |
10+ years | 83% | Salehrabi & Rotstein (2004) |
Success means the tooth remains functional without pain or infection signs. Failures usually occur within the first two years. After that, treated teeth perform reliably for decades.
Factors improving success:
Complete canal cleaning
Quality root filling
Timely crown placement
Good oral hygiene maintenance
How to Prevent Tooth Nerve Death?

Prevention focuses on early decay management, trauma protection, and good oral hygiene.
Preventive Strategies
Regular Dental Check-ups: Visit your dentist every six months. Professional cleanings remove plaque you miss at home. Examinations catch cavities early. Small fillings prevent pulp exposure. X-rays reveal decay between teeth that eyes cannot see.
Early Cavity Treatment: Do not wait for toothaches. Treat cavities when they are small and shallow. A simple filling costs less than a root canal. It preserves more natural tooth structure. It eliminates the risk of pulp necrosis from that cavity.
Mouthguards: Athletes need custom-fitted mouthguards. These absorb impact forces that crack teeth and kill nerves. People who grind their teeth need night guards. These prevent cracks and wear that lead to pulp exposure.
Proper Oral Hygiene: Brush twice daily with fluoride toothpaste. Floss between teeth daily. Fluoride strengthens enamel against acid attacks. Proper technique removes plaque from all tooth surfaces. Electric toothbrushes improve cleaning efficiency for many people.
Early Intervention Importance
Treat pulpitis before it becomes necrosis. Reversible pulpitis warns you to act. The sharp pain with cold drinks signals inflammation. Remove the cause, and the pulp recovers. Wait, and the inflammation becomes irreversible.
Monitor previously restored teeth. Large fillings age and leak. Cracks develop around old restorations. Regular examinations catch these problems early. Replacement restorations prevent bacterial invasion.
Tooth Nerve Death vs Other Dental Conditions

Pulp necrosis differs from reversible pulpitis and gum disease in severity and treatment needs.
Understanding the differences between dental conditions helps you recognize when you need urgent care:
Condition | Nerve Status | Pain Characteristics | Required Treatment | Urgency |
Reversible pulpitis | Alive, inflamed | Sharp, brief, stimulus-dependent | Filling or desensitization | Routine |
Irreversible pulpitis | Dying | Lingering, spontaneous, severe | Root canal or extraction | Urgent |
Pulp necrosis | Dead | Variable, may be painless | Root canal or extraction | Semi-urgent |
Periodontal disease | Variable | Gum-focused, chewing pain | Deep cleaning, surgery | Varies |
Dental abscess | Usually dead | Throbbing, swollen, systemic signs | Drainage + antibiotics + definitive treatment | Emergency |
Key Distinction: Reversible pulpitis represents a warning. Pulp necrosis represents failure to heed that warning. The treatments differ dramatically in complexity, cost, and tooth preservation.
Frequently Asked Questions
Does a Dead Tooth Always Hurt?
No. Many necrotic teeth cause no pain at all. The nerve dies, so it cannot transmit pain signals. However, the infection continues spreading silently. Eventually, pain returns when the infection affects surrounding tissues. Some people never feel pain despite advanced infection. Regular dental X-rays catch these silent cases.
Can a Dead Tooth Heal Itself?
No. Necrotic pulp tissue cannot regenerate. The blood supply does not reestablish spontaneously. Bacteria continue colonizing the dead tissue. The infection worsens without treatment. Professional intervention remains the only solution. Antibiotics provide temporary symptom relief but do not cure the underlying condition.
How Long Can a Dead Tooth Stay Untreated?
Time varies widely. Some necrotic teeth remain asymptomatic for months or years. Others develop acute infections within weeks. You cannot predict which course your tooth will take. Delay risks serious complications. The infection spreads to bone and soft tissues. Treatment becomes more complex and expensive. Tooth survival odds decrease.
Is Root Canal Treatment Painful?
Modern root canal therapy causes minimal discomfort. Local anesthesia numbs the tooth completely. You feel pressure but not pain. Post-treatment soreness resembles a bruise. It lasts one to two days. Over-the-counter medications manage this effectively. The procedure relieves the severe pain of pulp necrosis. Patients report that root canals hurt less than the toothache that preceded them.
Can a Dead Tooth Turn Black?
Yes. Discoloration represents a classic sign of pulp necrosis. Blood cells break down inside the tooth after the nerve dies. Hemoglobin releases iron compounds. These stain the dentin from within. The tooth appears grey, brown, or black depending on the breakdown products. Front teeth show this most obviously. Internal bleaching can lighten the tooth after root canal treatment.
Conclusion: Why Early Diagnosis Matters
Tooth nerve death is preventable and treatable, but delays increase the risk of infection, tooth loss, and systemic complications.
Tooth nerve death progresses through predictable stages. Your body provides warning signs. Sharp sensitivity signals reversible pulpitis. Lingering pain signals irreversible damage. Discoloration confirms nerve death. Each stage offers intervention opportunities.
Early diagnosis saves teeth. Small fillings prevent root canals. Timely root canals prevent extractions. Regular dental visits catch problems before symptoms start. Modern dentistry preserves natural teeth longer than ever before.
Prevention costs less than treatment. Good oral hygiene, regular check-ups, and prompt cavity treatment protect your pulp. Mouthguards prevent trauma-related necrosis. These simple measures maintain your natural smile for life.
If you suspect a dead tooth nerve, schedule a dental examination immediately. Do not wait for pain. Do not hope the problem resolves itself. Professional evaluation determines the best course of action. With proper care, even necrotic teeth can function normally for decades.
Your teeth serve you daily. Invest in their care. Protect their pulp. Preserve your oral health for a lifetime of confident smiles.
References
Bergenholtz, Gunnar. "Pathogenic Mechanisms in Pulpal Disease." Journal of Endodontics, vol. 45, no. 9, 2019, pp. S26-S31.
Cotti, Elisabetta, and Giovanni Campisi. "Advanced Radiographic Techniques for the Detection of Lesions in Bone." Endodontic Topics, vol. 24, no. 1, 2020, pp. 77-91.
Lockhart, Peter B., et al. "Poor Oral Health as a Risk Factor for Infective Endocarditis–Related Bacteremia." Journal of the American Dental Association, vol. 150, no. 4, 2019, pp. 286-294.
Ng, Yuan-Ling, et al. "Outcome of Primary Root Canal Treatment: Systematic Review of the Literature - Part 1. Effects of Study Characteristics on Probability of Healing." International Endodontic Journal, vol. 44, no. 10, 2011, pp. 891-902.
Plotino, Gianluca, et al. "Tooth Discoloration after Endodontic Treatment: A Review." Journal of Endodontics, vol. 43, no. 9, 2017, pp. 1467-1475.
Ricucci, Domenico, et al. "Correlation between Clinical and Histologic Pulp Diagnoses." Journal of Endodontics, vol. 44, no. 11, 2018, pp. 1685-1691.
Salehrabi, Reza, and Ilan Rotstein. "Endodontic Treatment Outcomes in a Large Patient Population in the USA: An Epidemiological Study." Journal of Endodontics, vol. 30, no. 12, 2004, pp. 846-850.
Siqueira, José F., and Isabela N. Rôças. "The Microbiome in Apical Periodontitis: Targeting the Microbial Etiology of Root Canal Infections." Journal of Oral Microbiology, vol. 12, no. 1, 2020, pp. 1-15.
Taha, Nasser A., and Abeer Abdellatif. "Comparison of the Accuracy of Periapical Radiography and Cone Beam Computed Tomography in the Diagnosis of Periapical Pathology." Australian Endodontic Journal, vol. 47, no. 1, 2021, pp. 110-118.



